Opportunistically get a baseline oxygen saturation reading for any patients likely to have chronically reduced saturations
There are four main aspects of managing mild to moderate COVID-19 in the community: patient advice and education on illness course (including red flag symptoms and timing); comfort medications and non-pharmacological comfort and hydration measures; management of comorbidities and other medications; and safety netting around red flag symptoms, and who and when to call.
Patient advice and education
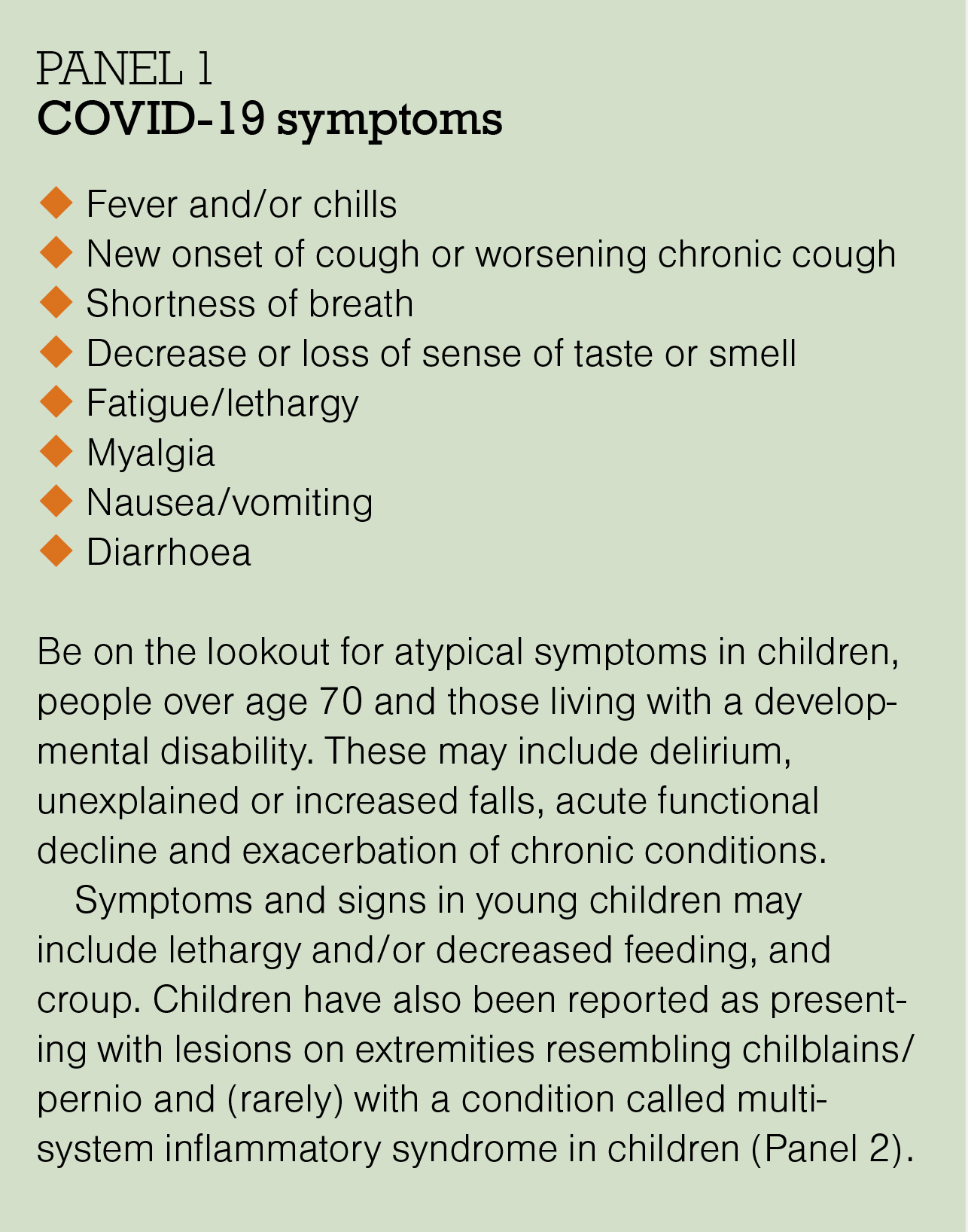
Set expectations – similar to influenza, COVID-19 most often has a longer recovery time than “a virus”. Explain that the typical symptoms are cough, fever and fatigue, but they may also have breathlessness, muscle aches, sore throat, headache, and loss of sense of smell and/or taste.
Rest – fatigue is often a marker for hypoxia, and experience with more unwell patients tells us increased mechanical work of breathing may lead to increased lung damage, so it makes sense not to do anything that triggers dyspnoea/tachycardia. If patients have pulse oximeters, they can measure oxygen saturation after different activities, which is a way to reinforce this message.
Change position to aid breathing – prone lying is used for inpatients, and while there is currently no evidence for outpatients, it makes sense to change positions to move secretions and change mechanical work of breathing and improve comfort.
Hydrate – give advice to ensure adequate hydration.
Next steps – give clear guidance on who to contact if symptoms (eg, breathlessness) get worse. For example, give the patient a self-monitoring checklist with a plan for deterioration, as well as details about the contact process.
Call 111 if:
- you have severe trouble breathing or severe chest pain
- you are very confused or not thinking clearly
- you pass out (lose consciousness).
Call the clinic* if:
- you have new or worse trouble breathing
- your symptoms are getting worse
- you start getting better and then get worse
- you have severe dehydration, such as having a very dry mouth, passing only a little urine, feeling very light-headed
- your oxygen saturation (for those with pulse oximeters), after rechecking, is below the level acceptable for you or if it changes by 3 per cent since the previous day – the care team will advise on acceptable levels, but generally, an oxygen saturation of 93 per cent or greater is acceptable.
* If you don’t provide 24-hour cover, make sure instructions for evenings and weekends are clear. A formal back-up arrangement is essential for those being actively monitored in the high-risk group.
More information – email or direct patients to the latest information on self-isolation or caring for someone with COVID-19, such as Health Navigator (tinyurl.com/HN-COVIDcare, which includes information for caregivers of children) and Unite against COVID-19 (tinyurl.com/Gov-COVIDcare). For those without access to email or internet, provide hard copies of useful resources.
A PDF providing information on illness course, breathing, red flags and pulse oximetry can be given to patients (tinyurl.com/COVIDPatientInfo).
Medications not indicated
As with most viral illnesses, there are few medications useful in outpatient treatment, and treatment options suggested on social media early in the pandemic have not been supported by evidence. As with all illnesses, a calm evidence-based approach to management is key, and, above all, avoiding harm, which includes avoiding unsupported treatments. There is now clearer evidence around many of the treatments initially suggested for COVID-19, and this evidence base is constantly growing.
It has been established that the following medications are not indicated for community COVID-19 care:
Hydroxychloroquine – should not be used. Recent studies indicate there is no evidence for benefit from azithromycin,1 hydroxychloroquine or the combination2 in outpatient management of COVID-19, in terms of time to recovery or risk of hospitalisation.
Antibiotics – should only be used if concomitant bacterial infection is suspected (in our experience, this is rare and presents as late deterioration) and the patient can be safely managed in the community. Usual antibiotic guidelines should be followed for uncomplicated or complicated bacterial pneumonia. Studies indicate there is no evidence for benefit from routine use of azithromycin1 or doxycycline3 (not surprising in a viral pneumonia).
Ivermectin – there is no convincing evidence for benefit on mortality, need for invasive mechanical ventilation, hospital admission, duration of hospitalisation or time to viral clearance.4
Oral steroids – should not be used in ambulant community-dwelling primary care patients. A meta-analysis shows the evidence for benefit is only in patients requiring oxygen. There is evidence that if used in milder cases (not requiring oxygen), mortality is increased.5
Think: COVID-19 is not like a COPD exacerbation.
Possibly helpful medications
Inhaled corticosteroids – there was initial uncertainty about the potential benefits and harms of ICS. A new, large randomised controlled trial in primary care patients at risk of more serious illness suggests ICS (budesonide was studied) could shorten the time to first self-reported recovery by an estimated median of 2.9 days (11.8 days in the ICS group versus 14.7 days in the usual care group). For the outcome of hospital admission or death, the trial did not achieve the superiority threshold for ICS versus usual care.6 There are meta-analyses under way that will help answer this question.
On the basis of these data, it seems reasonable to consider ICS use for early COVID-19 in patients similar to the trial population group (aged ≥65 with ongoing symptoms from COVID-19, or aged ≥50 with specific comorbidities – ie, the high-risk group) who are interested in using them (only 80 per cent of participants in the trial ICS group used them for at least a week).7
Analyses in this trial do not provide any pointers to who is most likely to benefit. Importantly, these trial data do not support use in younger populations who are at lower risk of complications (aged <65 with no comorbidities or anyone aged <50).
Further, because vaccination was uncommon in trial participants, an important question is what effect would be seen in fully vaccinated people, who have a different illness severity and trajectory.
Paracetamol – is a safer medication for symptoms than NSAIDs. This is not specific to COVID-19, but NSAIDs increase cardiovascular risk in any viral illness (tinyurl.com/HFAM-NSAIDs).
Other comfort remedies – can be used as usual if there is evidence for benefit in relieving viral illness symptoms (eg, honey for sore throat).
Other medications – are becoming available for treatment of high-risk groups (eg, monoclonal antibodies and other antiviral agents). It will be important to watch for emerging evidence on these, as well as licensing for use in New Zealand, to determine their role in evidence-based primary care management.
Note: this information is updated on hfam.ca as new evidence on management and treatments emerges. It can be found by checking the updates tab (hfam.ca/updates).
What about existing medications?
- Medications for COPD and asthma should be continued (tinyurl.com/HFAM-Resp).
- ACE inhibitors and angiotensin II receptor blockers appear safe to continue in COVID-19 despite early concerns (tinyurl.com/HFAM-ACE-ARB).
- If the patient is at risk of dehydration (eg, diarrhoea), think of their risk for acute kidney injury if they are taking medications such as an ACE inhibitor or ARB plus a diuretic plus aspirin – these may need pausing to avoid AKI, which is a significant feature of more severe COVID-19 illness (see detailed advice about common medications that may need to be paused at tinyurl.com/SADMANS).
- If the patient is on immunosuppressant medications, consult with the relevant specialist – they may need pausing.
Paediatric considerations
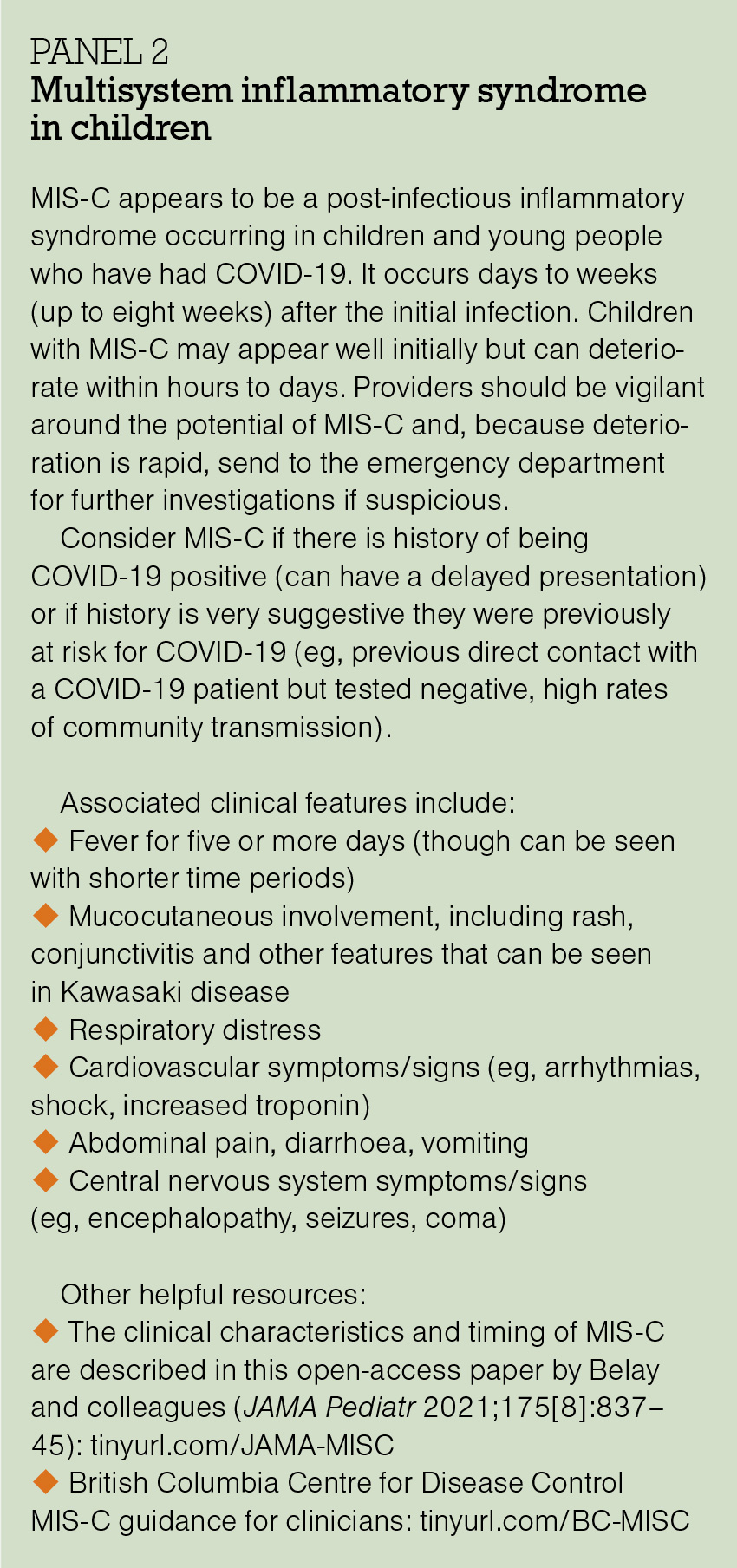
For children with COVID-19, approach care as you would for any viral illness – by screening for signs and symptoms of an unstable child. Video would be preferable to phone assessment if this is possible.
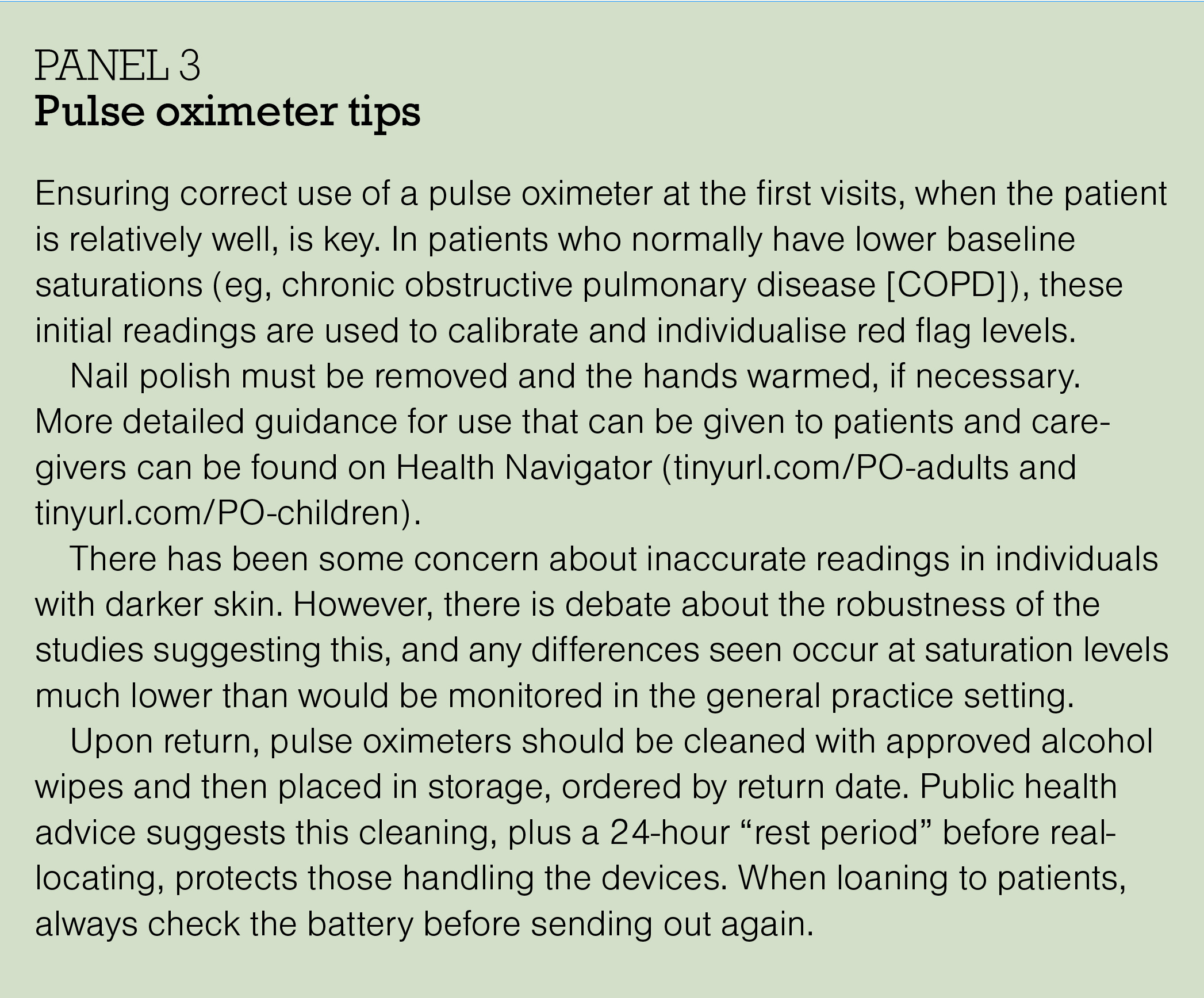
While adults and older children in average and high-risk categories should have a home pulse oximeter to assist monitoring, if available, paediatric experts recommend against specialist pulse oximeters for monitoring of younger children as these are difficult to use in an unwell child, are unreliable and may distract from other aspects of assessment.
Practicalities – what to do now to get ready
Familiarise yourself with your COVID-19 pathway, roles and responsibilities, and consider how you will connect with patients as early as possible in their illness trajectory and then systematically monitor them. Do you have a personal health record template ready to allow you to easily track change over time (eg, tinyurl.com/eChart-example)?
Develop a method such as a clinic register to track all currently active patients and ensure all scheduled monitoring appointments are completed. How will weekend monitoring be ensured when required?
Do a “walk through” of the scenario of monitoring a patient, including the roles different team members will take. For example, it is good if one or, ideally, two people (so there is built-in backup) take responsibility for holding a register of currently active patients and ensuring all follow-up visits are completed. How will positive patients be added to that register?
Engage the whole team – for example, reception staff need to know that if one of the actively monitored patients calls for advice outside their scheduled appointment time, they need to be promptly put through to a clinical team member (a crucial aspect of safety netting).
If you have capacity to do so now, try to clear your existing and near-future preventive and routine care activities that require in-person attendance, in case pressure on care means these get delayed. This includes routine blood test monitoring for chronic conditions, as increased community COVID-19 prevalence has substantial knock-on effects on availability of routine laboratory tests.
Where possible, opportunistically get a baseline oxygen saturation reading for any patients likely to have chronically reduced saturations (eg, COPD) and record it in the chart. This is very helpful when calibrating monitoring targets if they become unwell with COVID-19.
Act local – as well as your clinic team, the wider community team is also important. Models of care provision will depend on integration with other providers contributing to the COVID-19 response, in particular, public health and community organisations and volunteers. Is there a secondary care team or specialist service that is the designated local “who to call” resource for urgent advice? Do you know how to access them?
Effective local response means working together, with good communication, to provide the most efficient care. This ensures no one falls through the cracks of medical or social care, and it avoids duplication, given the human resource pressures COVID-19 puts on the health system. Think about key local stakeholders and resources to connect with now.
How will aspects of keeping patients safely in their homes be managed (eg, food security)? Where will patients be quickly transferred and cared for if their home environment is not suitable or stable? What local palliative services are available for frail patients who would not benefit from escalated care, which could enable them to die close to loved ones (eg, home oxygen providers, local palliative care teams)?
Conclusion
Population health outcomes are better when primary care is strongest, and COVID-19 is no exception. The generalist person-focused approach of primary care is essential in providing excellent care for those patients who do not need hospitalisation, and experienced clinical judgement in determining those who do. Primary care has wide reach across the community, and distribution of patients across providers means capacity is unlikely to be overwhelmed.
The value of familiarity in unfamiliar times cannot be underestimated either – being monitored by a known and trusted team is very reassuring, and knowledge of the patient and their situation facilitates attention to the physical, mental and psychological aspects of the care needed.









![Barbara Fountain, editor of New Zealand Doctor Rata Aotearoa, and Paul Hutchison, GP and senior medical clinician at Tāmaki Health [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/Barbara%20Fountain%2C%20editor%20of%20New%20Zealand%20Doctor%20Rata%20Aotearoa%2C%20and%20Paul%20Hutchison%2C%20GP%20and%20senior%20medical%20clinician%20at%20T%C4%81maki%20Health%20CR%20Simon%20Maude.jpg?itok=-HbQ1EYA)
![Lori Peters, NP and advanced health improvement practitioner at Mahitahi Hauora, and Jasper Nacilla, NP at The Terrace Medical Centre in Wellington [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/2.%20Lori%20Peters%2C%20NP%20and%20advanced%20HIP%20at%20Mahitahi%20Hauora%2C%20and%20Jasper%20Nacilla%2C%20NP%20at%20The%20Terrace%20Medical%20Centre%20in%20Wellington%20CR%20Simon%20Maude.jpg?itok=sUfbsSF1)
![Ministry of Social Development health and disability coordinator Liz Williams, regional health advisors Mary Mojel and Larah Takarangi, and health and disability coordinators Rebecca Staunton and Myint Than Htut [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/3.%20Ministry%20of%20Social%20Development%27s%20Liz%20Williams%2C%20Mary%20Mojel%2C%20Larah%20Takarangi%2C%20Rebecca%20Staunton%20and%20Myint%20Than%20Htut%20CR%20Simon%20Maude.jpg?itok=9ceOujzC)
![Locum GP Helen Fisher, with Te Kuiti Medical Centre NP Bridget Woodney [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/4.%20Locum%20GP%20Helen%20Fisher%2C%20with%20Te%20Kuiti%20Medical%20Centre%20NP%20Bridget%20Woodney%20CR%20Simon%20Maude.jpg?itok=TJeODetm)
![Ruby Faulkner, GPEP2, with David Small, GPEP3 from The Doctors Greenmeadows in Napier [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/5.%20Ruby%20Faulkner%2C%20GPEP2%2C%20with%20David%20Small%2C%20GPEP3%20from%20The%20Doctors%20Greenmeadows%20in%20Napier%20CR%20Simon%20Maude.jpg?itok=B0u4wsIs)
![Rochelle Langton and Libby Thomas, marketing advisors at the Medical Protection Society [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/6.%20Rochelle%20Langton%20and%20Libby%20Thomas%2C%20marketing%20advisors%20at%20the%20Medical%20Protection%20Society%20CR%20Simon%20Maude.jpg?itok=r52_Cf74)
![Specialist GP Lucy Gibberd, medical advisor at MPS, and Zara Bolam, urgent-care specialist at The Nest Health Centre in Inglewood [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/7.%20Specialist%20GP%20Lucy%20Gibberd%2C%20medical%20advisor%20at%20MPS%2C%20and%20Zara%20Bolam%2C%20urgent-care%20specialist%20at%20The%20Nest%20Health%20Centre%20in%20Inglewood%20CR%20Simon%20Maude.jpg?itok=z8eVoBU3)
![Olivia Blackmore and Trudee Sharp, NPs at Gore Health Centre, and Gaylene Hastie, NP at Queenstown Medical Centre [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/8.%20Olivia%20Blackmore%20and%20Trudee%20Sharp%2C%20NPs%20at%20Gore%20Health%20Centre%2C%20and%20Gaylene%20Hastie%2C%20NP%20at%20Queenstown%20Medical%20Centre%20CR%20Simon%20Maude.jpg?itok=Z6u9d0XH)
![Mary Toloa, specialist GP at Porirua and Union Community Health Service in Wellington, Mara Coler, clinical pharmacist at Tū Ora Compass Health, and Bhavna Mistry, specialist GP at Porirua and Union Community Health Service [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/9.%20Mary%20Toloa%2C%20Porirua%20and%20Union%20Community%20Health%20Service%20in%20Wellington%2C%20Mara%20Coler%2C%20T%C5%AB%20Ora%20Compass%20Health%2C%20and%20Bhavna%20Mistry%2C%20PUCHS%20CR%20Simon%20Maude.jpg?itok=kpChr0cc)