The strength of decision-making for patients with aortic stenosis lies in the recently evolved concept of the heart team
Once AVR is indicated, it should be performed promptly due to the ongoing risk of death, even in the short term. Options now include surgical (open-heart) AVR (SAVR) or transcatheter AVR (TAVR).
Surgical AVR
SAVR can be performed with either a bioprosthetic (tissue) valve or a mechanical one. In the absence of complications, patients typically spend one night in an intensive care unit and five to seven days in hospital following SAVR.
A bioprosthetic valve has the benefit of avoiding anticoagulation (unless otherwise indicated – eg, atrial fibrillation) but has the downside of limited durability. Most surgical bioprosthetic valves can be expected to last between 10 and 20 years, although this varies greatly depending on valve type and patient-related factors.4,5
To avoid the likelihood of valve degeneration requiring further intervention, most patients under age 50 receive a mechanical valve unless there are reasons to avoid anticoagulation with warfarin (eg, family planning, poor compliance, occupational hazards or other patient preferences).
Between ages 50 and 65, treatment choice is often individualised, depending on attitudes to anticoagulation and reintervention. Almost all patients over age 65 will have a bioprosthetic valve, considering that a transcatheter valve can now be placed inside a failed bioprosthesis, avoiding re-operative open-heart surgery.
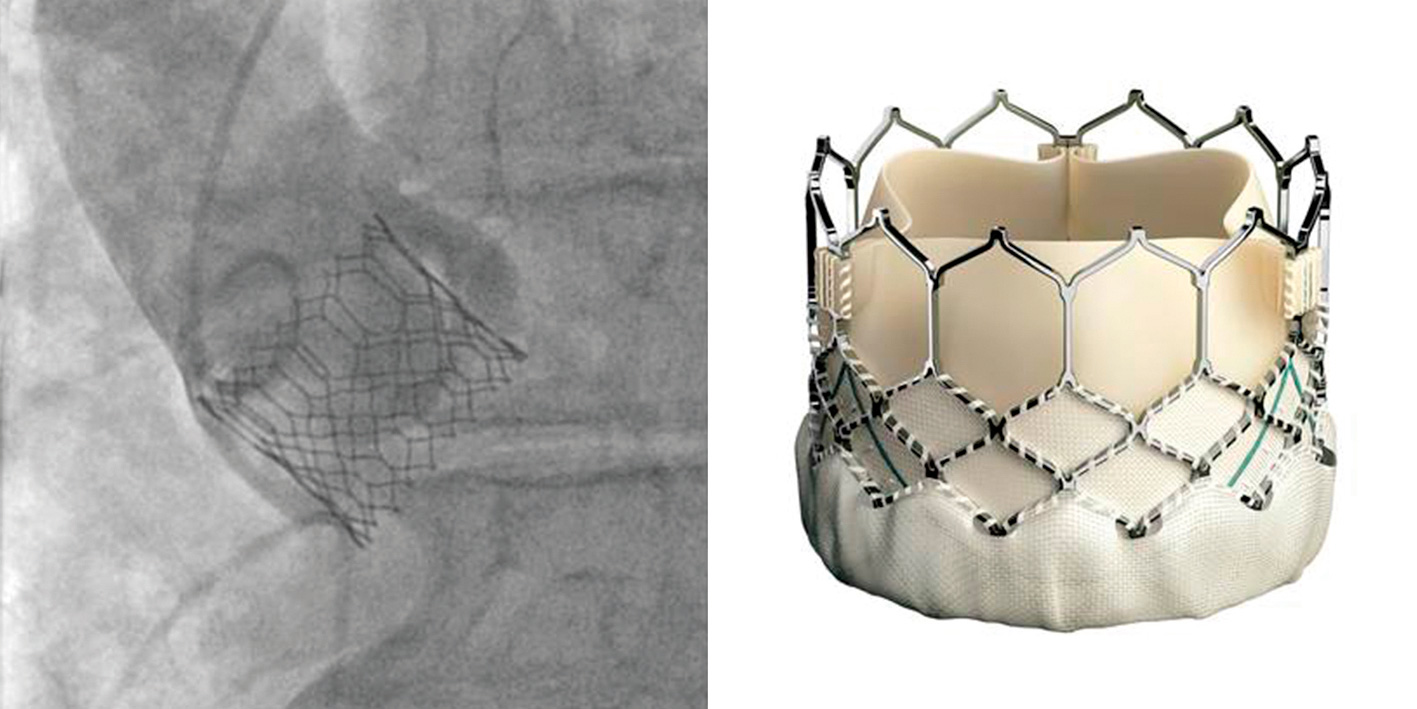
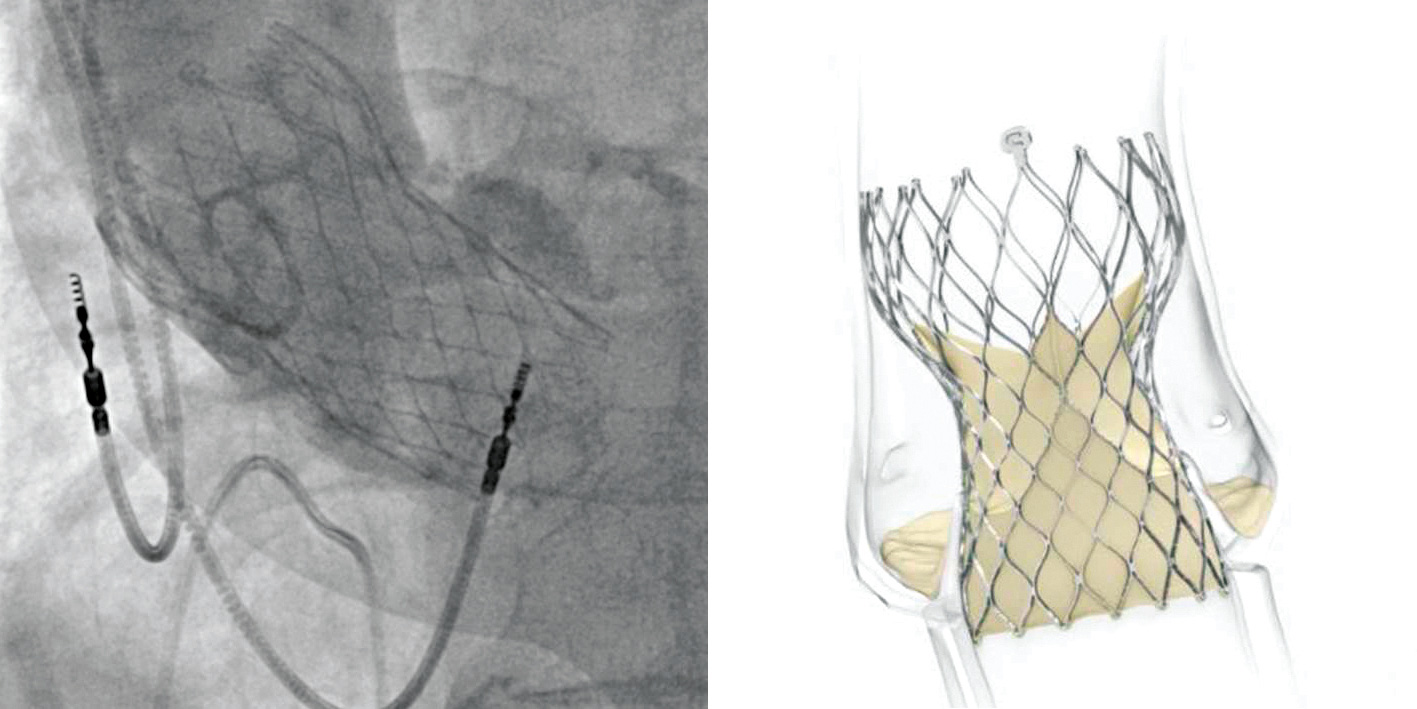
Transcatheter AVR
TAVR is a percutaneous procedure that has recently emerged as a safe and effective alternative to surgical bioprosthetic valves in carefully selected patients. Because TAVR has a shorter history, there are no data on very-long-term durability of these valves in younger patients.
In order to understand the evolution of this field, it is important to understand that, in clinical practice, patients with AS are classed according to their risk of death within 30 days of open-heart surgery. Patients are stratified into extreme (inoperable), high (>8 per cent risk of death), intermediate (4–8 per cent) and low-risk (<4 per cent) categories.
A typical high-risk patient would be in their 80s with several comorbidities, while intermediate-risk patients are typically those in their 80s with very mild comorbidity or those in their 70s with moderate comorbidity. Low-risk patients are typically those in their 70s or very early 80s with no other medical problems.
A series of randomised trials performed within the last 10 years has looked at the use of TAVR in patients of decreasing surgical risk. These trials began by comparing TAVR with medical therapy alone in patients in whom open-heart surgery was not possible due to extreme surgical risk. These studies showed a large reduction in the risk of death, improvement in symptoms and reduction in heart failure hospitalisation in those treated with TAVR.3
Subsequent trials tested TAVR against SAVR in progressively lower risk cohorts, with TAVR being shown to be safer and more cost-effective than open-heart surgery in high-risk patients.6,7
In intermediate-risk patients, TAVR and SAVR appear to be similar in terms of major adverse events, such as death and stroke, but with a much faster recovery and fewer hospital readmissions with TAVR.8,9
Recent randomised trials in carefully selected low-risk patients showed patients treated with either SAVR or TAVR had excellent outcomes, but with slightly lower incidence of stroke and death with TAVR than with SAVR. In this low-risk group, TAVR had other significant advantages, including fewer cases of atrial fibrillation, shorter hospital stays, fewer subsequent readmissions and improved symptoms and quality of life measures.10,11
One important limitation of these studies on low-risk patients is the currently short follow-up. Given the younger age and lack of comorbidity in these patients, long follow-up takes on much greater importance than in earlier trials.
Presently, transcatheter valves are significantly more expensive than surgical ones, although trial data suggest overall treatment costs still favour TAVR once adjusted for quality of life and other associated costs.12
Making treatment decisions – the heart team
Presently in New Zealand, there is variation in treatment pathways depending on geography and insurance coverage. TAVR is widely held as the treatment of choice for AS in older intermediate, high and extreme-risk patients in whom treatment is not considered futile (futility is covered below). Some DHBs offer TAVR to low-risk patients, while others currently do not.
The strength of decision-making for patients with AS lies in the recently evolved concept of the heart team – a multidisciplinary group of specialists that includes cardiac surgeons, cardiologists, intensive care specialists, nurse specialists and geriatricians.
Other than confirming the diagnosis of severe AS by echocardiography, the most important role of the heart team is to ensure safe and effective treatment of the aortic valve while appropriately managing other heart disease, such as concomitant coronary and mitral valve disease.
The risk of a TAVR procedure is largely dictated by anatomy, as evaluated by pre-procedural CT imaging, which forms the basis of most discussions once TAVR is planned. CT factors that increase procedural risk include calcification of the aortic annulus and heavily calcified iliofemoral arteries.
If arterial access is inadequate for the usual transfemoral approach, alternatives include access to the subclavian/axillary artery or direct surgical access to the aorta or LV apex itself. These are increasingly invasive, so must be considered in the context of comorbidities and overall goals of care, as well as the appropriateness of an open surgical alternative.
The role of the heart team has become increasingly important as younger and more complex patients are considered for treatment. Not only does short-term safety need to be considered but so too the longitudinal care of patients, given the potential for future reintervention. This is quite distinct to the early days of TAVR when the longitudinal care of patients was less important, given the advanced age and comorbid state of many patients in that era.
Although coronary and mitral valve disease may now be treated using percutaneous techniques, in younger, fitter patients, open-heart surgery may serve as a more comprehensive solution, albeit a more invasive one. As these decisions become increasingly complex, the strengths of all members of the heart team are increasingly drawn upon.
Futility – who should not be treated?
Besides the feasibility of TAVR in the treatment of AS, a great deal of what was learned from the early TAVR experience was an understanding of which patients do not thrive despite relief of aortic valve obstruction.
Futility not only refers to major complications from intervention but also the failure to improve in terms of functional status or quality of life.
The most common markers of futility are frailty (poor nutritional or functional status), oxygen dependence (indicating either a very advanced heart failure state or important lung disease), cognitive impairment and major competing non-cardiac comorbidity (eg, malignancy).13 The heart team is instrumental in careful assessment of these factors and establishing appropriate goals of care in such patients.









![Barbara Fountain, editor of New Zealand Doctor Rata Aotearoa, and Paul Hutchison, GP and senior medical clinician at Tāmaki Health [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/Barbara%20Fountain%2C%20editor%20of%20New%20Zealand%20Doctor%20Rata%20Aotearoa%2C%20and%20Paul%20Hutchison%2C%20GP%20and%20senior%20medical%20clinician%20at%20T%C4%81maki%20Health%20CR%20Simon%20Maude.jpg?itok=-HbQ1EYA)
![Lori Peters, NP and advanced health improvement practitioner at Mahitahi Hauora, and Jasper Nacilla, NP at The Terrace Medical Centre in Wellington [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/2.%20Lori%20Peters%2C%20NP%20and%20advanced%20HIP%20at%20Mahitahi%20Hauora%2C%20and%20Jasper%20Nacilla%2C%20NP%20at%20The%20Terrace%20Medical%20Centre%20in%20Wellington%20CR%20Simon%20Maude.jpg?itok=sUfbsSF1)
![Ministry of Social Development health and disability coordinator Liz Williams, regional health advisors Mary Mojel and Larah Takarangi, and health and disability coordinators Rebecca Staunton and Myint Than Htut [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/3.%20Ministry%20of%20Social%20Development%27s%20Liz%20Williams%2C%20Mary%20Mojel%2C%20Larah%20Takarangi%2C%20Rebecca%20Staunton%20and%20Myint%20Than%20Htut%20CR%20Simon%20Maude.jpg?itok=9ceOujzC)
![Locum GP Helen Fisher, with Te Kuiti Medical Centre NP Bridget Woodney [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/4.%20Locum%20GP%20Helen%20Fisher%2C%20with%20Te%20Kuiti%20Medical%20Centre%20NP%20Bridget%20Woodney%20CR%20Simon%20Maude.jpg?itok=TJeODetm)
![Ruby Faulkner, GPEP2, with David Small, GPEP3 from The Doctors Greenmeadows in Napier [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/5.%20Ruby%20Faulkner%2C%20GPEP2%2C%20with%20David%20Small%2C%20GPEP3%20from%20The%20Doctors%20Greenmeadows%20in%20Napier%20CR%20Simon%20Maude.jpg?itok=B0u4wsIs)
![Rochelle Langton and Libby Thomas, marketing advisors at the Medical Protection Society [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/6.%20Rochelle%20Langton%20and%20Libby%20Thomas%2C%20marketing%20advisors%20at%20the%20Medical%20Protection%20Society%20CR%20Simon%20Maude.jpg?itok=r52_Cf74)
![Specialist GP Lucy Gibberd, medical advisor at MPS, and Zara Bolam, urgent-care specialist at The Nest Health Centre in Inglewood [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/7.%20Specialist%20GP%20Lucy%20Gibberd%2C%20medical%20advisor%20at%20MPS%2C%20and%20Zara%20Bolam%2C%20urgent-care%20specialist%20at%20The%20Nest%20Health%20Centre%20in%20Inglewood%20CR%20Simon%20Maude.jpg?itok=z8eVoBU3)
![Olivia Blackmore and Trudee Sharp, NPs at Gore Health Centre, and Gaylene Hastie, NP at Queenstown Medical Centre [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/8.%20Olivia%20Blackmore%20and%20Trudee%20Sharp%2C%20NPs%20at%20Gore%20Health%20Centre%2C%20and%20Gaylene%20Hastie%2C%20NP%20at%20Queenstown%20Medical%20Centre%20CR%20Simon%20Maude.jpg?itok=Z6u9d0XH)
![Mary Toloa, specialist GP at Porirua and Union Community Health Service in Wellington, Mara Coler, clinical pharmacist at Tū Ora Compass Health, and Bhavna Mistry, specialist GP at Porirua and Union Community Health Service [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/9.%20Mary%20Toloa%2C%20Porirua%20and%20Union%20Community%20Health%20Service%20in%20Wellington%2C%20Mara%20Coler%2C%20T%C5%AB%20Ora%20Compass%20Health%2C%20and%20Bhavna%20Mistry%2C%20PUCHS%20CR%20Simon%20Maude.jpg?itok=kpChr0cc)