In New Zealand, all infants with an abnormal red reflex or a family history of inherited ocular disorders should be referred for a comprehensive ophthalmic examination.22,23
The sensitivity of the red reflex test is limited as it is a screening tool – when compared with a comprehensive eye examination, a sensitivity of 99.6 per cent for anterior segment disease (cornea, iris and lens) but only 4.1 per cent for posterior segment disease (structures behind the lens) was reported.24 However, in practice, case detection is probably lower than these reported figures.
In the UK, where red reflex screening is standard practice, a retrospective review of congenital cataract detection indicated that by eight weeks of age, only 47 per cent of cases had been identified.25
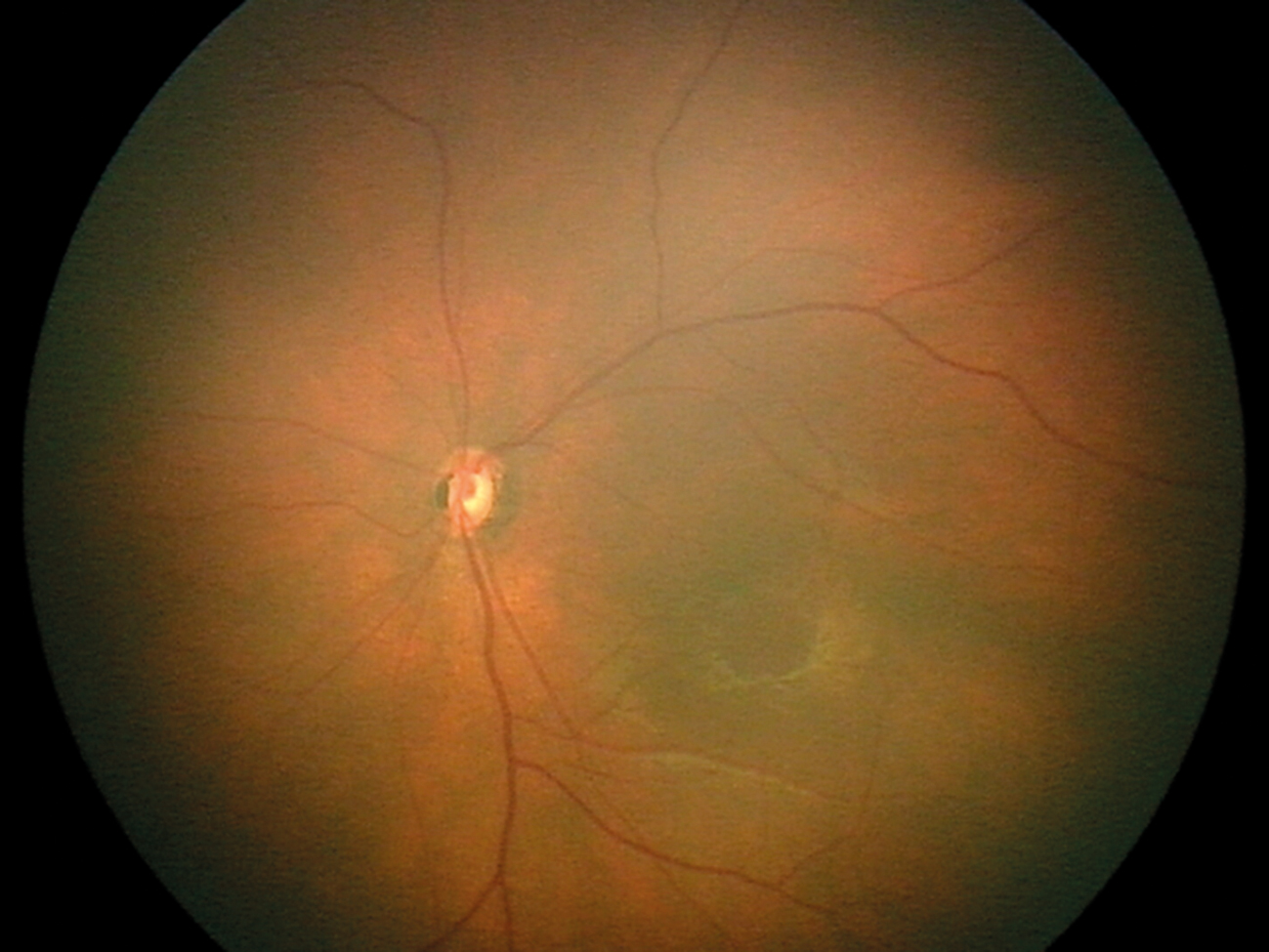
For posterior segment disease detection, a study of dilated red reflex examination of 37 paediatric eyes by a paediatric ophthalmologist failed to detect any of the 13 cases of retinoblastoma in an at-risk group.26
Reasons for the reduced detection rates are likely multifactorial and, in all likelihood, related to inadequate training,27 incorrect implementation of the red reflex test,28 as well as the sensitivity of the test itself.24
Therefore, without overcoming logistical, test sensitivity and educational challenges, vision-impairing ocular opacities and posterior segment disease may still be missed.25
However, the red reflex test remains a very useful screening tool when performed appropriately.
The red reflex test can also be useful for older children and even adults to check the clarity of the ocular media, but this should be used in conjunction with visual acuity measurements, observance of visual behaviour, and gross ocular assessment with an ophthalmoscope.
Visual acuity measurement
Visual acuity is the key measure of clarity of vision. Visual acuity starts at approximately 0.15 logMAR (6/180) at one month of age and develops to adult-equivalent vision of 0.0 logMAR (6/6) by five years.29,30
Methods for assessing this varying vision must be age and developmental stage appropriate:
- Preferential looking techniques, such as Cardiff or Teller cards, are appropriate for preverbal or cognitively impaired children.29,31
- The LEA Symbols Test is appropriate for preschool children, with a success rate of 76 per cent at age three and 95 per cent at age four, as well as high comparability to the Landolt C.32
- Compliance with quantitative letter-based acuity testing can be achieved in the majority of cognitively normal five-year-olds.31
- The ETDRS chart (developed for the Early Treatment Diabetic Retinopathy Study) has high repeatability measures in school-aged children with refractive errors.33
In all measures of visual acuity with a chart, ensure it is well lit, the child is at the appropriate distance away and the chart has maintained its contrast. Record the visual acuity, eye used, whether aided or unaided, distance of measurement and type of chart used.
In general practice, it is not common to have a large range of visual acuity tests available; therefore, using the tools you have available in the appropriate manner, and referring when further information is required, is recommended. Continually praising children encourages them to maintain focus and attempt smaller optotypes during threshold visual acuity testing.
When only a letter chart is available for a young child, you can consider using a matching card – a printed card with the letters on it – for the child to match to rather than needing to name the letters. These can be particularly helpful with shy children.
In even younger children, assessment of fixing and following at a set, recorded distance is appropriate. A small, colourful toy is an excellent tool to use for this.
In addition, a simple “objection to occlusion” test can be used. The child’s eyes are covered in turn with the palm of your hand, and equal objection to occluding them is a “normal” result. The amount of protest is often child dependent, so comparison of protest is the measure.
For example, a child with severely reduced vision in the right eye will not protest much when the right eye is covered; however, if the left eye is covered, they will protest as you have covered up their main view of the world. This difference in response is recorded as “unequal objection to occlusion” and indicates a possible difference in vision between the eyes, requiring referral for further assessment.
When referring cases and reduced vision is suspected, a visual acuity measurement is beneficial – ideally both binocular and monocular results. If not possible, then simply stating “concern of reduced visual acuity in both/right/left eye(s)” is suitable.
In a clinical setting, it is important to have a low threshold for referral of paediatric ocular conditions for further detailed examination.
B4 School Vision Screening
Reduced visual acuity and uncorrected refractive error (myopia, hyperopia or astigmatism) impact on academic performance, including reduced early literacy scores.34
B4 School Vision Screening is undertaken by vision and hearing technicians between a child’s fourth and fifth birthdays. Increased accuracy of screening has been reported with increasing age, and this may be due to the visual acuity letter test.
The screening is designed to detect amblyopia; however, due to the nature of the screening test, it also detects reduced distance vision from other causes. Hyperopia (long-sightedness) and strabismus (eye turns) are often not detected through this screening test.18
If bilateral reduced vision or a significant difference between the eyes is detected, then referral for optometric or ophthalmic examination is warranted, with exact referral guidelines varying between DHBs.
B4 School Vision Screening is important to diagnose and treat children with reduced distance visual acuity, but will not capture all children requiring refractive correction. In the case of myopia, most children who go on to develop myopia will not have developed it in time to be detected at this early screening.
Change in refraction with age is expected and is part of normal growth and emmetropisation (the minimisation of refractive error) of the eye. Infants are born hyperopic with an average axial length less than 17mm. The majority of ocular growth occurs before 24 months, and the emmetropisation process is completed between six and eight years of age.35 However, refractive error can continue to change throughout childhood for some children, leading to myopia.
Key support services
Vision is a key sense for function, development and education. From birth, vision develops throughout childhood. Therefore, it is important to detect anything impacting on this development and to either treat or support children with visual impairment. In addition to local optometric and ophthalmic services, there are specific support services for children with visual impairment.
Blind Low Vision NZ (blindlowvision.org.nz) is the national charity supporting all New Zealanders, not just children, who are blind or have low vision. Blind Low Vision NZ provides counselling services, orientation and mobility, and has an amazing library of alternative access books. Referral criteria for Blind Low Vision NZ are a visual acuity of 6/24 or worse in the better eye, or significantly reduced peripheral vision. There is no age restriction.
Blind Low Vision NZ has a specialist team to provide cultural support to Pacific clients, while Kāpō Māori Aotearoa provides cultural services for Māori clients. Kāpō Māori Aotearoa (kapomaori.com) is a national kaupapa Māori provider of peer support and health and disability services. It is a member-based society open to all people (disabled, able-bodied, Māori and non-Māori) and has an established reputation in the blindness community.
The key service for children is the Blind and Low Vision Education Network NZ (BLENNZ; blennz.school.nz), which is part of the Ministry of Education. BLENNZ is a school made up of a national network of educational services for ākonga (learners) who are blind, deafblind or have low vision. It provides a range of services, including teaching support in schools, orientation and mobility, low vision aids, specific immersion courses, and a specialist transdisciplinary national assessment when required.
BLENNZ supports children and young people with low vision and blindness to achieve their potential in education. Referral criteria for BLENNZ are a visual acuity of 6/18 or worse in the better eye, significantly reduced peripheral vision, or cerebral visual impairment affecting curriculum access.
The Ministry of Education has funding via the Ongoing Resourcing Scheme specifically for children with reduced vision. BLENNZ organises ORS applications and support for these children.
Other support groups available include Parents of Vision Impaired (pvi.org.nz). PVI is made up of parents of children who are blind or visually impaired, who aim to support other parents in the same position. They provide shared experience, support and advocacy from their unique experience and perspective.
The GP can also provide referral for treatment and refractive correction. A relationship with the local optometrist and ophthalmologist with paediatric interests can be a fantastic resource in managing this patient population.










![Barbara Fountain, editor of New Zealand Doctor Rata Aotearoa, and Paul Hutchison, GP and senior medical clinician at Tāmaki Health [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/Barbara%20Fountain%2C%20editor%20of%20New%20Zealand%20Doctor%20Rata%20Aotearoa%2C%20and%20Paul%20Hutchison%2C%20GP%20and%20senior%20medical%20clinician%20at%20T%C4%81maki%20Health%20CR%20Simon%20Maude.jpg?itok=-HbQ1EYA)
![Lori Peters, NP and advanced health improvement practitioner at Mahitahi Hauora, and Jasper Nacilla, NP at The Terrace Medical Centre in Wellington [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/2.%20Lori%20Peters%2C%20NP%20and%20advanced%20HIP%20at%20Mahitahi%20Hauora%2C%20and%20Jasper%20Nacilla%2C%20NP%20at%20The%20Terrace%20Medical%20Centre%20in%20Wellington%20CR%20Simon%20Maude.jpg?itok=sUfbsSF1)
![Ministry of Social Development health and disability coordinator Liz Williams, regional health advisors Mary Mojel and Larah Takarangi, and health and disability coordinators Rebecca Staunton and Myint Than Htut [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/3.%20Ministry%20of%20Social%20Development%27s%20Liz%20Williams%2C%20Mary%20Mojel%2C%20Larah%20Takarangi%2C%20Rebecca%20Staunton%20and%20Myint%20Than%20Htut%20CR%20Simon%20Maude.jpg?itok=9ceOujzC)
![Locum GP Helen Fisher, with Te Kuiti Medical Centre NP Bridget Woodney [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/4.%20Locum%20GP%20Helen%20Fisher%2C%20with%20Te%20Kuiti%20Medical%20Centre%20NP%20Bridget%20Woodney%20CR%20Simon%20Maude.jpg?itok=TJeODetm)
![Ruby Faulkner, GPEP2, with David Small, GPEP3 from The Doctors Greenmeadows in Napier [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/5.%20Ruby%20Faulkner%2C%20GPEP2%2C%20with%20David%20Small%2C%20GPEP3%20from%20The%20Doctors%20Greenmeadows%20in%20Napier%20CR%20Simon%20Maude.jpg?itok=B0u4wsIs)
![Rochelle Langton and Libby Thomas, marketing advisors at the Medical Protection Society [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/6.%20Rochelle%20Langton%20and%20Libby%20Thomas%2C%20marketing%20advisors%20at%20the%20Medical%20Protection%20Society%20CR%20Simon%20Maude.jpg?itok=r52_Cf74)
![Specialist GP Lucy Gibberd, medical advisor at MPS, and Zara Bolam, urgent-care specialist at The Nest Health Centre in Inglewood [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/7.%20Specialist%20GP%20Lucy%20Gibberd%2C%20medical%20advisor%20at%20MPS%2C%20and%20Zara%20Bolam%2C%20urgent-care%20specialist%20at%20The%20Nest%20Health%20Centre%20in%20Inglewood%20CR%20Simon%20Maude.jpg?itok=z8eVoBU3)
![Olivia Blackmore and Trudee Sharp, NPs at Gore Health Centre, and Gaylene Hastie, NP at Queenstown Medical Centre [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/8.%20Olivia%20Blackmore%20and%20Trudee%20Sharp%2C%20NPs%20at%20Gore%20Health%20Centre%2C%20and%20Gaylene%20Hastie%2C%20NP%20at%20Queenstown%20Medical%20Centre%20CR%20Simon%20Maude.jpg?itok=Z6u9d0XH)
![Mary Toloa, specialist GP at Porirua and Union Community Health Service in Wellington, Mara Coler, clinical pharmacist at Tū Ora Compass Health, and Bhavna Mistry, specialist GP at Porirua and Union Community Health Service [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/9.%20Mary%20Toloa%2C%20Porirua%20and%20Union%20Community%20Health%20Service%20in%20Wellington%2C%20Mara%20Coler%2C%20T%C5%AB%20Ora%20Compass%20Health%2C%20and%20Bhavna%20Mistry%2C%20PUCHS%20CR%20Simon%20Maude.jpg?itok=kpChr0cc)