In July 2020, I found myself unexpectedly in a mental health crisis. On the surface, life was “normal” – I was a typical millennial who had returned from overseas and relocated to Auckland for a new job and a fresh start. However, in my head, all was not well.
I was juggling a lot: COVID-19 had created job uncertainty, and I was losing a grandparent, managing family assets, and trying to keep on top of the daily grind during Auckland’s lockdowns.
It started small. At first, I was unable to relax. I lost my appetite and found myself overwhelmed with anxiety one day during a run.
One night, I was cooking dinner and was struck with a sudden thought: what if I hurt someone with this knife? My husband, who was in the same room as me, became the centre of that disturbing thought. I put the knife down and backed away. I thought, what the hell is wrong with me? Where did this come from? Am I a monster?
It was the start of a terrifying spiral. The more I tried to get rid of the thought, the stronger it became. I stopped sleeping, afraid that I would lose control in my sleep. Then, one night, there were some stories on the news – a murder and a sexual crime. I nearly vomited. What if I did that? Could I ever be capable?
I had a full-blown identity crisis. Thoughts that were contrary to my values looped continuously in my head. OCD is dubbed the “doubter’s disease”, and I wasn’t sure I knew who I was any more.
By now, I was panicking and hastily registered with a local medical centre. What came next was a blur of appointments and confusion as I became increasingly unwell. I couldn’t see my GP at short notice and had some horrendous experiences before I was referred to specialist mental health care.
I’m still haunted by one consult. It was with an unfamiliar doctor, and I hadn’t slept in days. I blurted out that I was really struggling with thoughts that I could harm others, and that I couldn’t bear to live with what was in my head anymore. I still remember the look of intense disgust that crossed his face, the raised eyebrows, and the judgemental exchange that followed. It was humiliating.
Alarmingly, I left with more sleeping pills than would be considered safe for someone who was suicidal. I felt he had confirmed my worst fears – that there was something deeply wrong with me, and that I didn’t deserve to live. What this doctor doesn’t realise is that a 15-minute consult nearly made me end my life that day. I came frighteningly close, and I still have nightmares about the experience.
I’m grateful that on the next call, I encountered a GP who was genuinely concerned for my wellbeing and recognised how much I was struggling. While no one had yet recognised OCD, this time, I was met with empathy and referred swiftly to the crisis team. I was initially diagnosed with “severe anxiety characterised by intrusive thoughts”.
Upon further deterioration, I was admitted to a respite service where a psychiatrist listened to the relentless disturbing thoughts I’d been plagued with. It took her about 20 minutes to diagnose OCD.
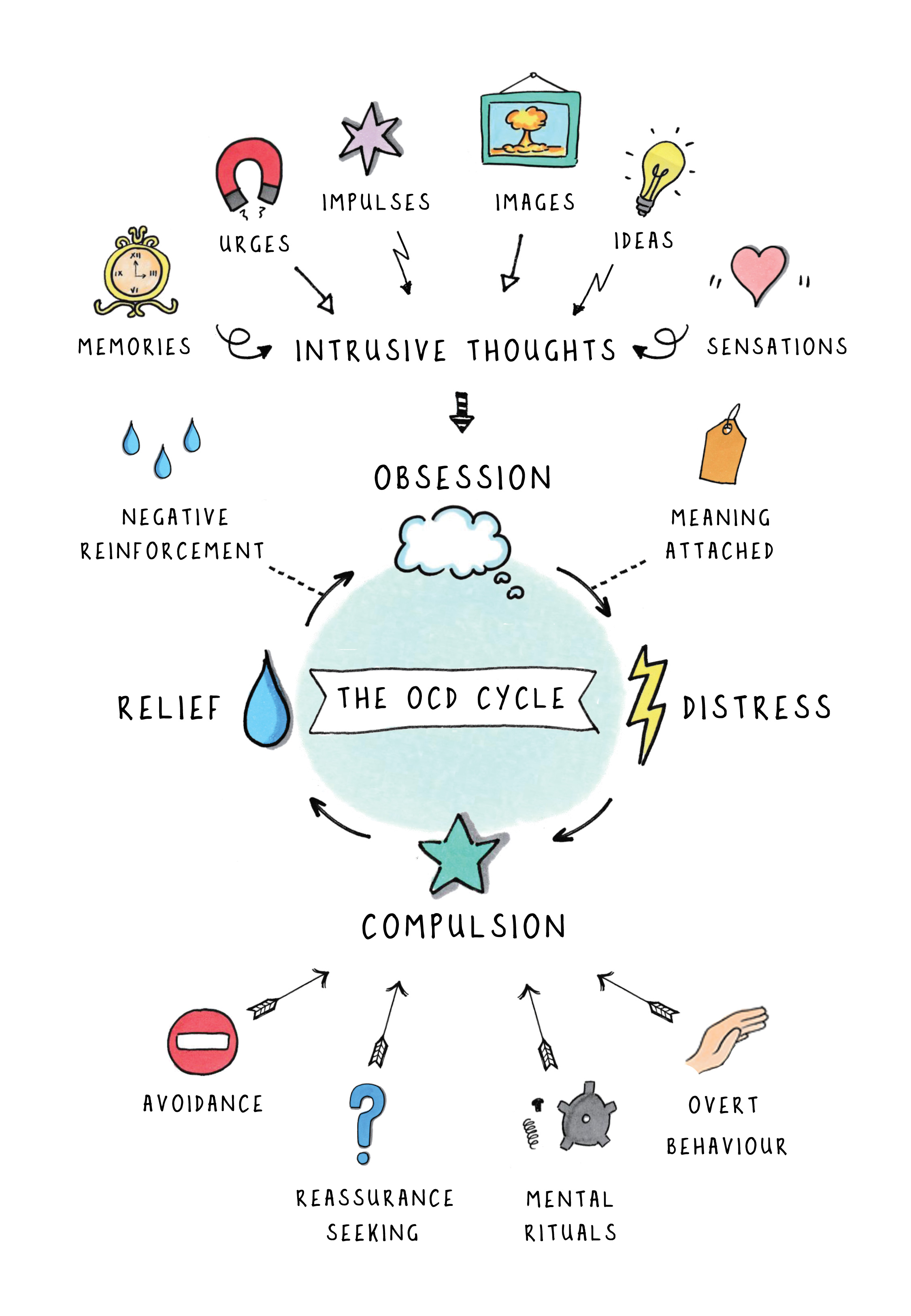
Like the general population, my understanding of OCD prior to diagnosis was poor. Unbeknown to me, I have the type of OCD that very few talk about – where one is haunted by ego-dystonic intrusive thoughts. It is nicknamed “Pure O” (or purely obsessional) because of the absence of visible compulsions.
I do not exhibit any of the stereotypical compulsions – no handwashing, no ordering, no rituals. Instead, my compulsions are primarily mental – the most obvious being reassurance seeking and searching for evidence that I’m not a “bad” person. My obsession of causing harm to others is common, but because of the way I presented, OCD wasn’t recognised until it was nearly too late.
My recovery wasn’t straightforward. I was in the public system for months, trialling multiple medications before finally finding one that worked. After several attempts, I was fortunate to find a clinical psychologist experienced in treating OCD with Exposure and Response Prevention (ERP) therapy. It has been incredibly challenging and expensive, but it has worked.
OCD is incredibly difficult to live with – no one wants to be tortured by their most feared thoughts every day. It also takes immense courage to share these experiences with a medical professional. So, even if you are alarmed by what your patient shares, acknowledgement of distress and basic empathy go a long way. I hope these words will reach the professionals who can make a tangible difference in the recovery of those living with OCD.





![Barbara Fountain, editor of New Zealand Doctor Rata Aotearoa, and Paul Hutchison, GP and senior medical clinician at Tāmaki Health [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/Barbara%20Fountain%2C%20editor%20of%20New%20Zealand%20Doctor%20Rata%20Aotearoa%2C%20and%20Paul%20Hutchison%2C%20GP%20and%20senior%20medical%20clinician%20at%20T%C4%81maki%20Health%20CR%20Simon%20Maude.jpg?itok=-HbQ1EYA)
![Lori Peters, NP and advanced health improvement practitioner at Mahitahi Hauora, and Jasper Nacilla, NP at The Terrace Medical Centre in Wellington [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/2.%20Lori%20Peters%2C%20NP%20and%20advanced%20HIP%20at%20Mahitahi%20Hauora%2C%20and%20Jasper%20Nacilla%2C%20NP%20at%20The%20Terrace%20Medical%20Centre%20in%20Wellington%20CR%20Simon%20Maude.jpg?itok=sUfbsSF1)
![Ministry of Social Development health and disability coordinator Liz Williams, regional health advisors Mary Mojel and Larah Takarangi, and health and disability coordinators Rebecca Staunton and Myint Than Htut [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/3.%20Ministry%20of%20Social%20Development%27s%20Liz%20Williams%2C%20Mary%20Mojel%2C%20Larah%20Takarangi%2C%20Rebecca%20Staunton%20and%20Myint%20Than%20Htut%20CR%20Simon%20Maude.jpg?itok=9ceOujzC)
![Locum GP Helen Fisher, with Te Kuiti Medical Centre NP Bridget Woodney [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/4.%20Locum%20GP%20Helen%20Fisher%2C%20with%20Te%20Kuiti%20Medical%20Centre%20NP%20Bridget%20Woodney%20CR%20Simon%20Maude.jpg?itok=TJeODetm)
![Ruby Faulkner, GPEP2, with David Small, GPEP3 from The Doctors Greenmeadows in Napier [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/5.%20Ruby%20Faulkner%2C%20GPEP2%2C%20with%20David%20Small%2C%20GPEP3%20from%20The%20Doctors%20Greenmeadows%20in%20Napier%20CR%20Simon%20Maude.jpg?itok=B0u4wsIs)
![Rochelle Langton and Libby Thomas, marketing advisors at the Medical Protection Society [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/6.%20Rochelle%20Langton%20and%20Libby%20Thomas%2C%20marketing%20advisors%20at%20the%20Medical%20Protection%20Society%20CR%20Simon%20Maude.jpg?itok=r52_Cf74)
![Specialist GP Lucy Gibberd, medical advisor at MPS, and Zara Bolam, urgent-care specialist at The Nest Health Centre in Inglewood [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/7.%20Specialist%20GP%20Lucy%20Gibberd%2C%20medical%20advisor%20at%20MPS%2C%20and%20Zara%20Bolam%2C%20urgent-care%20specialist%20at%20The%20Nest%20Health%20Centre%20in%20Inglewood%20CR%20Simon%20Maude.jpg?itok=z8eVoBU3)
![Olivia Blackmore and Trudee Sharp, NPs at Gore Health Centre, and Gaylene Hastie, NP at Queenstown Medical Centre [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/8.%20Olivia%20Blackmore%20and%20Trudee%20Sharp%2C%20NPs%20at%20Gore%20Health%20Centre%2C%20and%20Gaylene%20Hastie%2C%20NP%20at%20Queenstown%20Medical%20Centre%20CR%20Simon%20Maude.jpg?itok=Z6u9d0XH)
![Mary Toloa, specialist GP at Porirua and Union Community Health Service in Wellington, Mara Coler, clinical pharmacist at Tū Ora Compass Health, and Bhavna Mistry, specialist GP at Porirua and Union Community Health Service [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/9.%20Mary%20Toloa%2C%20Porirua%20and%20Union%20Community%20Health%20Service%20in%20Wellington%2C%20Mara%20Coler%2C%20T%C5%AB%20Ora%20Compass%20Health%2C%20and%20Bhavna%20Mistry%2C%20PUCHS%20CR%20Simon%20Maude.jpg?itok=kpChr0cc)