Opportunistically, you can have the biggest impact in fall prevention
Opportunistically, you can have the biggest impact in fall prevention. Ask all your older patients about falls, trips, slips and injuries all the time. What you don’t know can hurt them, and you will miss opportunities if you don’t ask: how many falls have you had in the last 12 months? Any injuries? How is your confidence about mobility?
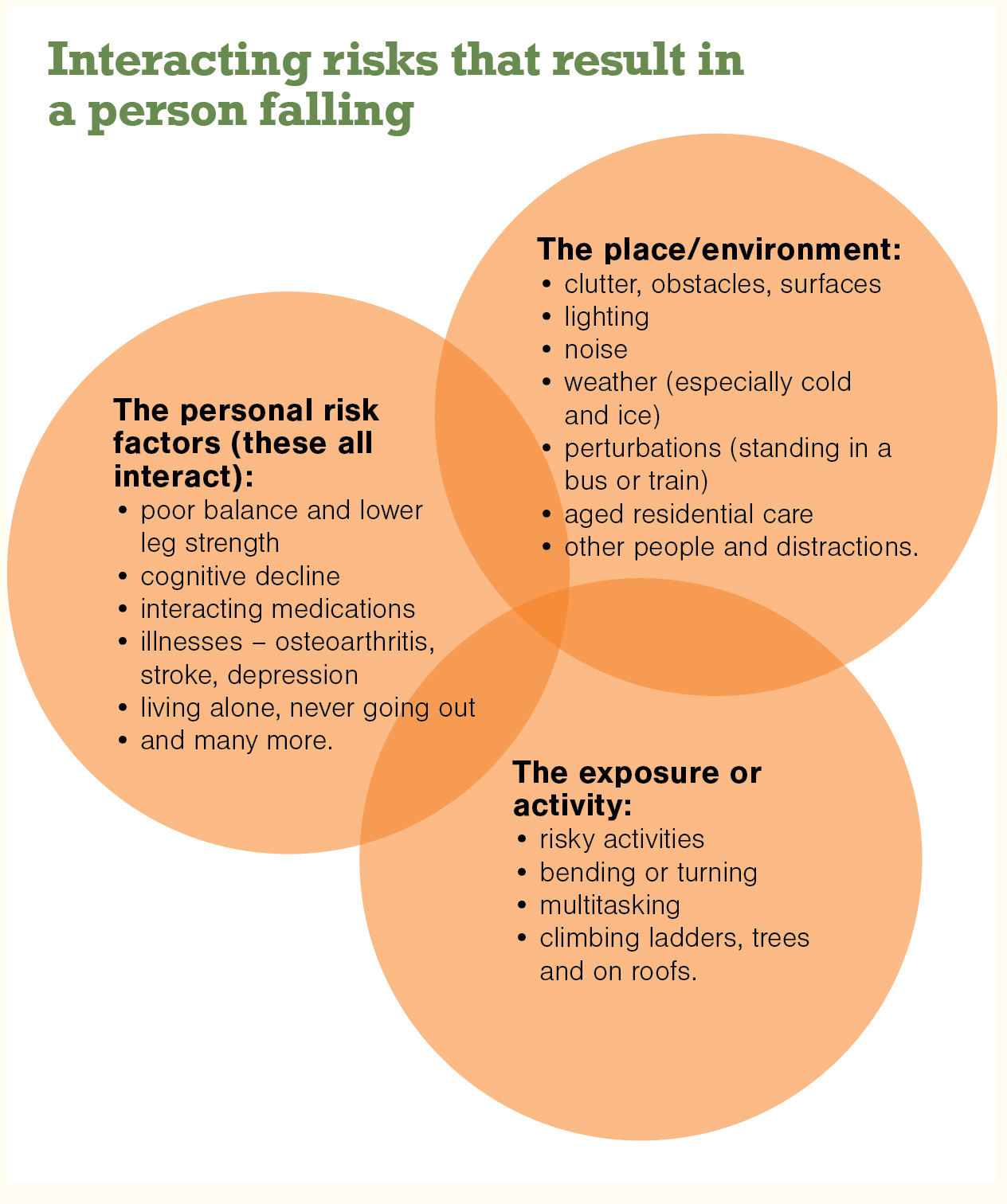
Remember the dynamic risk Venn diagram and talk to your patients. This kind of framework can lead to very useful discussion (patient education, self-management), especially while discussing “what happened”. Medical condition optimisation and medication review are mandatory. Preventing future falls is the objective, so promote behaviour modification, assist with understanding that risk plays a role, and give a firm idea about what works.
There have been hundreds of trials on fall prevention in the community. 6,7 There is overwhelming support for exercise in the form of lower-leg strengthening and balance retraining, using individual or group delivery and via several forms for those living in the community. Thai chi is also effective.
ACC accredits community strength and balance programmes as part of the Live Stronger for Longer programme (livestronger.org.nz), and there are thousands available around New Zealand. Most DHBs have a way for GPs to refer patients directly. In-home, one-on-one delivery for those who are home bound is also available in most DHBs.
The new aspect of activity programmes is perturbation training – actively tripping older people to reactivate reaction responses.8 Please don’t try this at home! It needs to be done with protection in place and will be available in some places via a special treadmill or a walking track, with sudden tripping devices randomly activated.
Home hazard modification through occupational therapist assessment is effective and accessible through older peoples’ health services from all DHBs.
Medical review and some specific medical interventions (eg, pacemaker insertion for those with carotid hypersensitivity), comprehensive geriatric assessment and intervention, combined with home occupational therapist referral for those with a falls injury resulting in emergency department attendance are effective. Medication review and modification by GPs reduces falls.
Attention to correction of visual impairment due to cataracts also reduces falls, and switching from multifocals to single-lens glasses helps; however, new glasses seem to increase the risk of falls. Footwear improvement can help, especially in icy places.
Multifactorial interventions (several of these strategies at once) are helpful, especially if there is an individualised risk assessment to direct the interventions.
For those in aged residential care, vitamin D supplementation and increasing protein and calories in the daily diet prevents falls and fractures.9,10
Specially designed gym equipment used under direction of a physiotherapist, with additional balance exercises, reduced falls in one trial. This HUR (Helsinki University Research) computerised air pressure equipment is available in New Zealand in at least one site.
Overall, GPs and nurse practitioners in primary care can have a large impact on falls in older people. The long-term support from the primary care provider, along with referral, coordination of prevention and rehabilitation will make a difference to outcomes related to falls and injury.






![Barbara Fountain, editor of New Zealand Doctor Rata Aotearoa, and Paul Hutchison, GP and senior medical clinician at Tāmaki Health [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/Barbara%20Fountain%2C%20editor%20of%20New%20Zealand%20Doctor%20Rata%20Aotearoa%2C%20and%20Paul%20Hutchison%2C%20GP%20and%20senior%20medical%20clinician%20at%20T%C4%81maki%20Health%20CR%20Simon%20Maude.jpg?itok=-HbQ1EYA)
![Lori Peters, NP and advanced health improvement practitioner at Mahitahi Hauora, and Jasper Nacilla, NP at The Terrace Medical Centre in Wellington [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/2.%20Lori%20Peters%2C%20NP%20and%20advanced%20HIP%20at%20Mahitahi%20Hauora%2C%20and%20Jasper%20Nacilla%2C%20NP%20at%20The%20Terrace%20Medical%20Centre%20in%20Wellington%20CR%20Simon%20Maude.jpg?itok=sUfbsSF1)
![Ministry of Social Development health and disability coordinator Liz Williams, regional health advisors Mary Mojel and Larah Takarangi, and health and disability coordinators Rebecca Staunton and Myint Than Htut [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/3.%20Ministry%20of%20Social%20Development%27s%20Liz%20Williams%2C%20Mary%20Mojel%2C%20Larah%20Takarangi%2C%20Rebecca%20Staunton%20and%20Myint%20Than%20Htut%20CR%20Simon%20Maude.jpg?itok=9ceOujzC)
![Locum GP Helen Fisher, with Te Kuiti Medical Centre NP Bridget Woodney [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/4.%20Locum%20GP%20Helen%20Fisher%2C%20with%20Te%20Kuiti%20Medical%20Centre%20NP%20Bridget%20Woodney%20CR%20Simon%20Maude.jpg?itok=TJeODetm)
![Ruby Faulkner, GPEP2, with David Small, GPEP3 from The Doctors Greenmeadows in Napier [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/5.%20Ruby%20Faulkner%2C%20GPEP2%2C%20with%20David%20Small%2C%20GPEP3%20from%20The%20Doctors%20Greenmeadows%20in%20Napier%20CR%20Simon%20Maude.jpg?itok=B0u4wsIs)
![Rochelle Langton and Libby Thomas, marketing advisors at the Medical Protection Society [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/6.%20Rochelle%20Langton%20and%20Libby%20Thomas%2C%20marketing%20advisors%20at%20the%20Medical%20Protection%20Society%20CR%20Simon%20Maude.jpg?itok=r52_Cf74)
![Specialist GP Lucy Gibberd, medical advisor at MPS, and Zara Bolam, urgent-care specialist at The Nest Health Centre in Inglewood [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/7.%20Specialist%20GP%20Lucy%20Gibberd%2C%20medical%20advisor%20at%20MPS%2C%20and%20Zara%20Bolam%2C%20urgent-care%20specialist%20at%20The%20Nest%20Health%20Centre%20in%20Inglewood%20CR%20Simon%20Maude.jpg?itok=z8eVoBU3)
![Olivia Blackmore and Trudee Sharp, NPs at Gore Health Centre, and Gaylene Hastie, NP at Queenstown Medical Centre [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/8.%20Olivia%20Blackmore%20and%20Trudee%20Sharp%2C%20NPs%20at%20Gore%20Health%20Centre%2C%20and%20Gaylene%20Hastie%2C%20NP%20at%20Queenstown%20Medical%20Centre%20CR%20Simon%20Maude.jpg?itok=Z6u9d0XH)
![Mary Toloa, specialist GP at Porirua and Union Community Health Service in Wellington, Mara Coler, clinical pharmacist at Tū Ora Compass Health, and Bhavna Mistry, specialist GP at Porirua and Union Community Health Service [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/9.%20Mary%20Toloa%2C%20Porirua%20and%20Union%20Community%20Health%20Service%20in%20Wellington%2C%20Mara%20Coler%2C%20T%C5%AB%20Ora%20Compass%20Health%2C%20and%20Bhavna%20Mistry%2C%20PUCHS%20CR%20Simon%20Maude.jpg?itok=kpChr0cc)