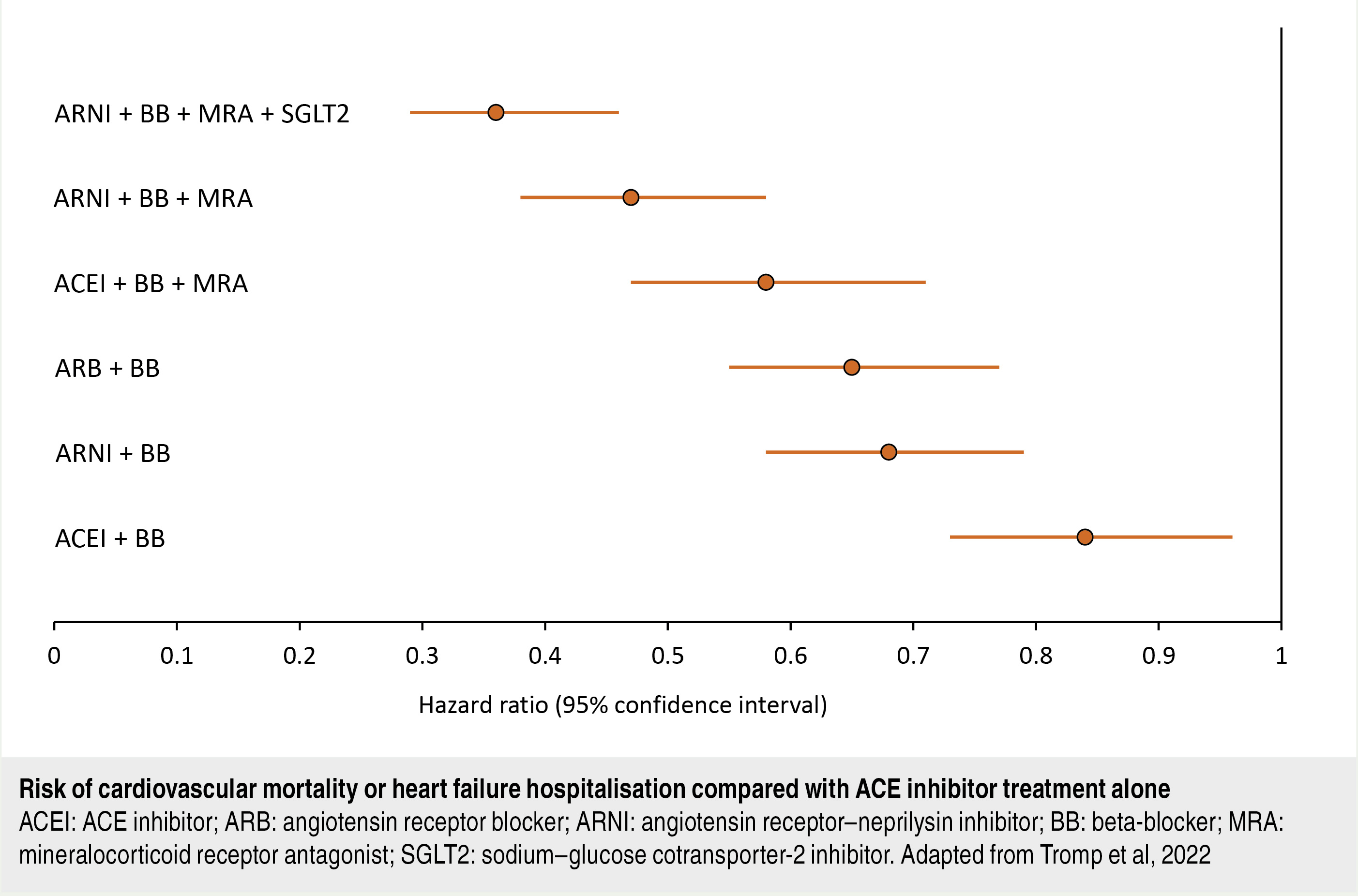
Every heart failure phenotype has a risk of progression and adverse cardiovascular events, especially without optimal treatment
How will this work?
You still have questions about how this process will work in primary care.
How does the hospital-orientated STRONG-HF study convert to a primary care environment?
The concept of high-intensity care is established, but understandably, this may take a little longer in general practice. However, it will likely be easier to initiate the four pillars in a person who is stable and has not just been hospitalised with an exacerbation of heart failure.
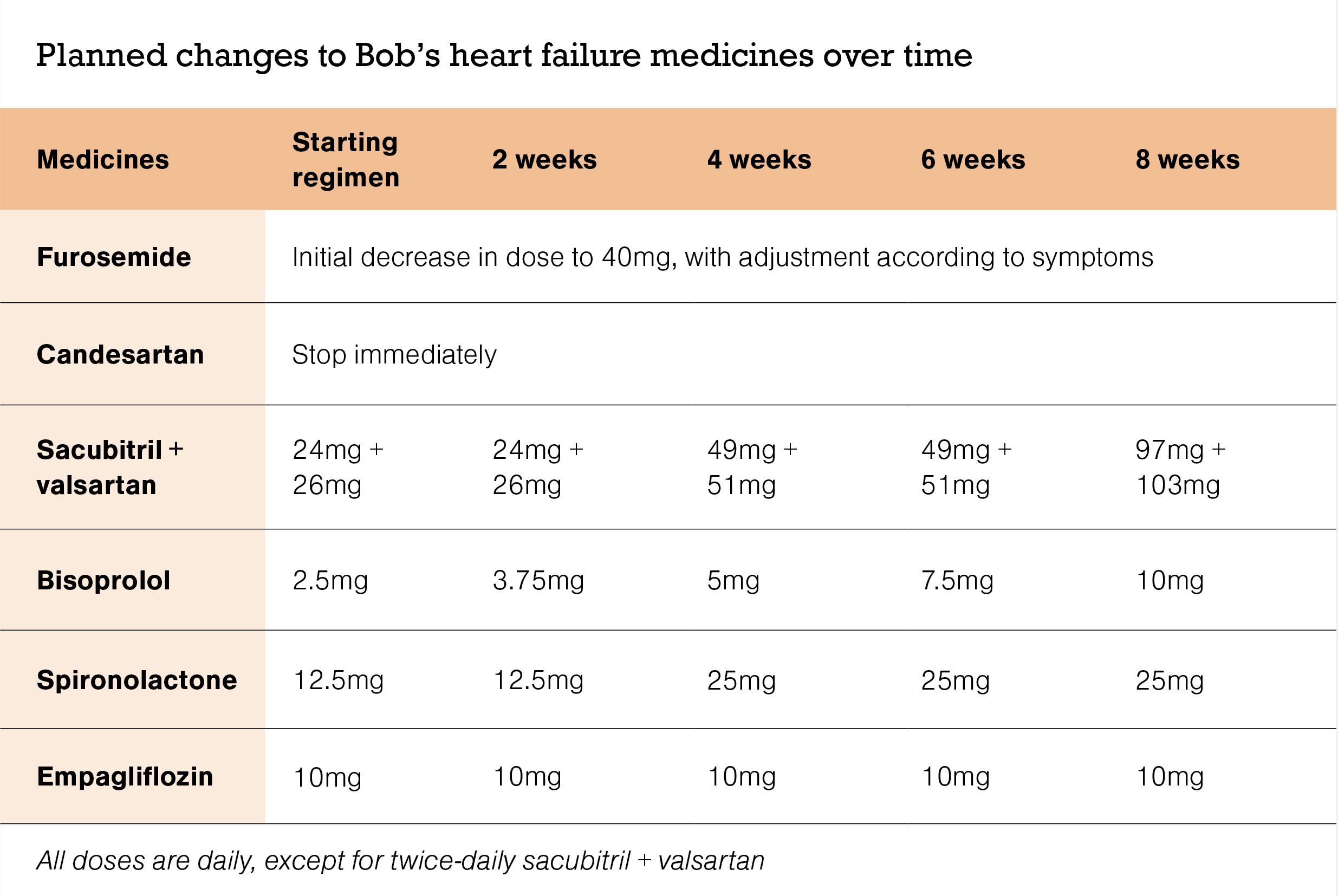
The four pillars can be initiated in primary care (compared with when beta-blockers and ACE inhibitors first became guideline-directed therapy and had to be started in hospital), but perhaps a little more conservatively – for example, initially aim for optimisation over six to 12 weeks, depending on the starting point for the person.
What about appointment time? Engagement could be a long process, especially if the person with heart failure is relatively well.
A study of patient perspectives found approximately 75 per cent of people with heart failure wanted more information on the condition and its consequences, prognosis and treatment. GPs are a preferred source of information.7 Having a crib sheet with brief notes would be helpful.
The term heart failure makes it sound like the heart is no longer working and there is nothing that can be done. Actually, heart failure means the heart isn’t pumping as well as it should. There is also a misconception that heart failure can reach a “stable” state, and that people who are doing well do not need all therapies. However, every heart failure phenotype has a risk of progression and adverse cardiovascular events, especially without optimal treatment.
Medical caregivers need to understand and convey these messages to patients. Start the conversation early about heart “decline” as opposed to failure. At the time of diagnosis, there is the opportunity for a medicines therapy plan to be discussed with all patients.
Obtaining written information, such as from the Heart Foundation (heartfoundation.org.nz) or Healthify He Puna Waiora (healthify.nz/health-a-z/h/heart-failure), can be helpful. The first appointment may need to be a double appointment, or you can consider spreading this information over two or three appointments using the wider team, as resources allow.
How do we organise frequent primary care monitoring and follow-up (cost, personnel)?
This can be a major barrier for some people with heart failure – there is the time required for the appointments and travel to the clinic, coupled with the potential cost of visits.
Setting expectations is important, as implementing the four pillars involves six to 12 weeks of close monitoring and medication changes. Hence, the person needs to have a good understanding of the benefits that will occur, the monitoring required and the planned titration. Involving the wider whānau is proven and recommended.
Follow-up may be done via video, telephone or even email – a quick “touching base” to reduce the time commitment. If the person has a blood pressure monitoring machine and good-quality scales at home, this is much less time-consuming for you and them. Involving others (eg, medical care assistants, kaiawhina) for some of the clinical variable monitoring with report back can be helpful, as is collaboration with Māori and Pacific health providers.
Brief follow-up consultations may help reduce the cost, or perhaps a “package of care” cost would be acceptable. Ideally, the PHO would invest in heart failure as a clinical quality indicator and factor in the extra time.
Other clinicians could also assist – the practice-based clinical advisory pharmacist, pharmacist prescriber or nurse practitioner could monitor and titrate the medicines, and this has been successful elsewhere.
In the long term, intense input when the diagnosis of heart failure is made and optimisation of pharmacotherapy with the four pillars would mean fewer acute visits for exacerbations of heart failure.
How will you identify people with heart failure?
Doing a practice management system query for people with heart failure will identify those who will benefit and be the first pass of a clinical audit. As you work through the list while you gain experience, you could start with the people in whom the least medicine changes are necessary, while recognising the most significant benefit is in those at greatest risk. Initially, while establishing the system, gaining clinical confidence and finding the most valuable resources, less complexity is preferable. You can discuss self-funding with those who do not meet the Special Authority criteria for this combination of medicines.








![Barbara Fountain, editor of New Zealand Doctor Rata Aotearoa, and Paul Hutchison, GP and senior medical clinician at Tāmaki Health [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/Barbara%20Fountain%2C%20editor%20of%20New%20Zealand%20Doctor%20Rata%20Aotearoa%2C%20and%20Paul%20Hutchison%2C%20GP%20and%20senior%20medical%20clinician%20at%20T%C4%81maki%20Health%20CR%20Simon%20Maude.jpg?itok=-HbQ1EYA)
![Lori Peters, NP and advanced health improvement practitioner at Mahitahi Hauora, and Jasper Nacilla, NP at The Terrace Medical Centre in Wellington [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/2.%20Lori%20Peters%2C%20NP%20and%20advanced%20HIP%20at%20Mahitahi%20Hauora%2C%20and%20Jasper%20Nacilla%2C%20NP%20at%20The%20Terrace%20Medical%20Centre%20in%20Wellington%20CR%20Simon%20Maude.jpg?itok=sUfbsSF1)
![Ministry of Social Development health and disability coordinator Liz Williams, regional health advisors Mary Mojel and Larah Takarangi, and health and disability coordinators Rebecca Staunton and Myint Than Htut [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/3.%20Ministry%20of%20Social%20Development%27s%20Liz%20Williams%2C%20Mary%20Mojel%2C%20Larah%20Takarangi%2C%20Rebecca%20Staunton%20and%20Myint%20Than%20Htut%20CR%20Simon%20Maude.jpg?itok=9ceOujzC)
![Locum GP Helen Fisher, with Te Kuiti Medical Centre NP Bridget Woodney [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/4.%20Locum%20GP%20Helen%20Fisher%2C%20with%20Te%20Kuiti%20Medical%20Centre%20NP%20Bridget%20Woodney%20CR%20Simon%20Maude.jpg?itok=TJeODetm)
![Ruby Faulkner, GPEP2, with David Small, GPEP3 from The Doctors Greenmeadows in Napier [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/5.%20Ruby%20Faulkner%2C%20GPEP2%2C%20with%20David%20Small%2C%20GPEP3%20from%20The%20Doctors%20Greenmeadows%20in%20Napier%20CR%20Simon%20Maude.jpg?itok=B0u4wsIs)
![Rochelle Langton and Libby Thomas, marketing advisors at the Medical Protection Society [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/6.%20Rochelle%20Langton%20and%20Libby%20Thomas%2C%20marketing%20advisors%20at%20the%20Medical%20Protection%20Society%20CR%20Simon%20Maude.jpg?itok=r52_Cf74)
![Specialist GP Lucy Gibberd, medical advisor at MPS, and Zara Bolam, urgent-care specialist at The Nest Health Centre in Inglewood [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/7.%20Specialist%20GP%20Lucy%20Gibberd%2C%20medical%20advisor%20at%20MPS%2C%20and%20Zara%20Bolam%2C%20urgent-care%20specialist%20at%20The%20Nest%20Health%20Centre%20in%20Inglewood%20CR%20Simon%20Maude.jpg?itok=z8eVoBU3)
![Olivia Blackmore and Trudee Sharp, NPs at Gore Health Centre, and Gaylene Hastie, NP at Queenstown Medical Centre [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/8.%20Olivia%20Blackmore%20and%20Trudee%20Sharp%2C%20NPs%20at%20Gore%20Health%20Centre%2C%20and%20Gaylene%20Hastie%2C%20NP%20at%20Queenstown%20Medical%20Centre%20CR%20Simon%20Maude.jpg?itok=Z6u9d0XH)
![Mary Toloa, specialist GP at Porirua and Union Community Health Service in Wellington, Mara Coler, clinical pharmacist at Tū Ora Compass Health, and Bhavna Mistry, specialist GP at Porirua and Union Community Health Service [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/9.%20Mary%20Toloa%2C%20Porirua%20and%20Union%20Community%20Health%20Service%20in%20Wellington%2C%20Mara%20Coler%2C%20T%C5%AB%20Ora%20Compass%20Health%2C%20and%20Bhavna%20Mistry%2C%20PUCHS%20CR%20Simon%20Maude.jpg?itok=kpChr0cc)