Patients with prostate cancer are seen every day in general practice. At each stage – from the decision to investigate for cancer right through to palliative care for advancing metastatic disease – GPs see it all. And the statistics reflect this. In New Zealand, prostate cancer is the most common cancer in men and the second most common cause of cancer death. In 2018 (the latest census data), 4176 men were diagnosed with prostate cancer and 495 men died from it.
Yet, for such an important public health issue, there remains considerable controversy and numerous frequently raised questions surrounding prostate cancer:
- Don’t all men die with prostate cancer rather than from the condition?
- Does early detection confer any benefit, or does it just lead to overtreatment and side effects?
- Who needs treatment and who should avoid it?
Currently, in New Zealand, there is no recommendation for population-based screening for prostate cancer. This stance is echoed in all major urological and cancer society guidelines throughout the world.
Screening is often viewed as a “dirty word” in relation to the prostate. At an individual level, if diagnosed with stage I or II prostate cancer, survival is close to 100 per cent at five years, but if diagnosed at stage IV, the survival rate is about 50 per cent at five years. However, population screening must clearly show – for the whole population, not just the individual – a health benefit by reducing either morbidity or mortality while minimising harm and being cost-effective.
The challenge in prostate cancer is that the time from early detection to symptoms or death is, for most men, greater than 10 years. Running trials and following men for such a long time, and accounting for competing morbidity, has made the evidence difficult to interpret.
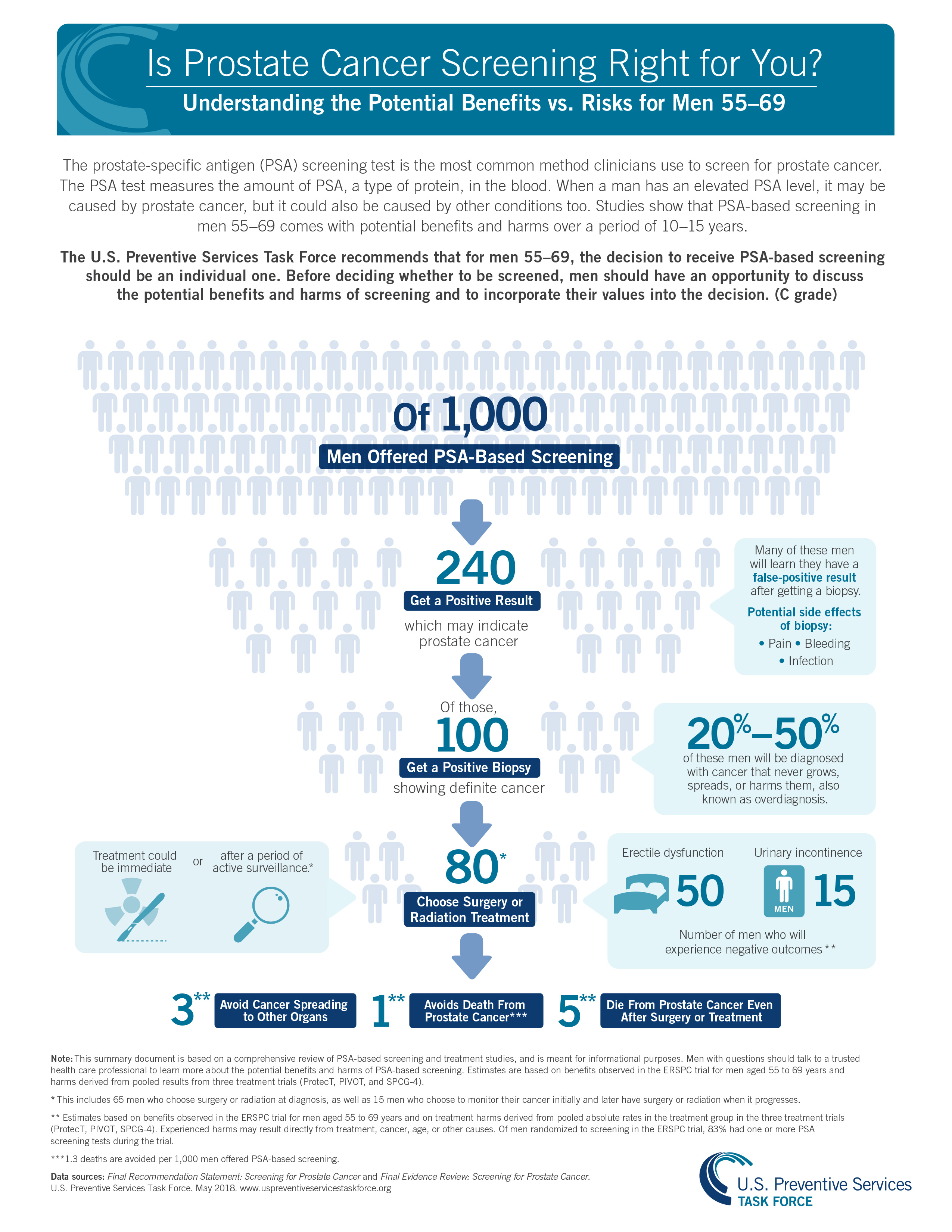
Current evidence from large, population-based, randomised controlled trials shows a reduction in prostate cancer mortality but no change in all-cause mortality with prostate cancer screening. Specifically, at 13 years, it is possible to prevent 1.3 deaths and three cases of metastatic disease for every 1000 men screened (Figure 1). This, however, comes at the expense of overdiagnosis and overtreatment for potentially 20 per cent of the men diagnosed with cancer. With further follow-up of this trial at 18 years, the number needed to screen and treat to prevent death continues to drop. This highlights the slow growth rate of prostate cancer as well as its importance with our ageing population.
In 2018, the US Preventive Services Task Force changed its grade D recommendation (no role for screening for prostate cancer) to a grade C recommendation (shared decision-making) for men aged 55 to 69. This change resulted from a reassessment of the updated evidence and an increasing awareness of the flaws and study population contamination of the large US screening trial. The task force is currently updating its recommendations again.
Current New Zealand recommendations on prostate cancer screening can be obtained from the Ministry of Health’s Prostate Cancer Management and Referral Guidance (tinyurl.com/MOH-prostate). The recommendation is for a shared decision-making process between health professional and patient. This should involve a discussion of the benefits and risks of screening.
This discussion almost exclusively occurs in primary care, with the GP responsible for trying to fit this into a standard appointment. Decision-making aids can be helpful but finding the ideal one can be difficult. Unfortunately, there is no one-size-fits-all guideline for every patient. Kupe is a tool sponsored by the Ministry of Health that attempts to provide support for this (kupe.net.nz). There are direct links on some patient management systems. Patients these days are efficient in using the internet and should be encouraged to seek out and learn from good-quality, up-to-date patient advocacy websites.











![Barbara Fountain, editor of New Zealand Doctor Rata Aotearoa, and Paul Hutchison, GP and senior medical clinician at Tāmaki Health [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/Barbara%20Fountain%2C%20editor%20of%20New%20Zealand%20Doctor%20Rata%20Aotearoa%2C%20and%20Paul%20Hutchison%2C%20GP%20and%20senior%20medical%20clinician%20at%20T%C4%81maki%20Health%20CR%20Simon%20Maude.jpg?itok=-HbQ1EYA)
![Lori Peters, NP and advanced health improvement practitioner at Mahitahi Hauora, and Jasper Nacilla, NP at The Terrace Medical Centre in Wellington [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/2.%20Lori%20Peters%2C%20NP%20and%20advanced%20HIP%20at%20Mahitahi%20Hauora%2C%20and%20Jasper%20Nacilla%2C%20NP%20at%20The%20Terrace%20Medical%20Centre%20in%20Wellington%20CR%20Simon%20Maude.jpg?itok=sUfbsSF1)
![Ministry of Social Development health and disability coordinator Liz Williams, regional health advisors Mary Mojel and Larah Takarangi, and health and disability coordinators Rebecca Staunton and Myint Than Htut [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/3.%20Ministry%20of%20Social%20Development%27s%20Liz%20Williams%2C%20Mary%20Mojel%2C%20Larah%20Takarangi%2C%20Rebecca%20Staunton%20and%20Myint%20Than%20Htut%20CR%20Simon%20Maude.jpg?itok=9ceOujzC)
![Locum GP Helen Fisher, with Te Kuiti Medical Centre NP Bridget Woodney [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/4.%20Locum%20GP%20Helen%20Fisher%2C%20with%20Te%20Kuiti%20Medical%20Centre%20NP%20Bridget%20Woodney%20CR%20Simon%20Maude.jpg?itok=TJeODetm)
![Ruby Faulkner, GPEP2, with David Small, GPEP3 from The Doctors Greenmeadows in Napier [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/5.%20Ruby%20Faulkner%2C%20GPEP2%2C%20with%20David%20Small%2C%20GPEP3%20from%20The%20Doctors%20Greenmeadows%20in%20Napier%20CR%20Simon%20Maude.jpg?itok=B0u4wsIs)
![Rochelle Langton and Libby Thomas, marketing advisors at the Medical Protection Society [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/6.%20Rochelle%20Langton%20and%20Libby%20Thomas%2C%20marketing%20advisors%20at%20the%20Medical%20Protection%20Society%20CR%20Simon%20Maude.jpg?itok=r52_Cf74)
![Specialist GP Lucy Gibberd, medical advisor at MPS, and Zara Bolam, urgent-care specialist at The Nest Health Centre in Inglewood [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/7.%20Specialist%20GP%20Lucy%20Gibberd%2C%20medical%20advisor%20at%20MPS%2C%20and%20Zara%20Bolam%2C%20urgent-care%20specialist%20at%20The%20Nest%20Health%20Centre%20in%20Inglewood%20CR%20Simon%20Maude.jpg?itok=z8eVoBU3)
![Olivia Blackmore and Trudee Sharp, NPs at Gore Health Centre, and Gaylene Hastie, NP at Queenstown Medical Centre [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/8.%20Olivia%20Blackmore%20and%20Trudee%20Sharp%2C%20NPs%20at%20Gore%20Health%20Centre%2C%20and%20Gaylene%20Hastie%2C%20NP%20at%20Queenstown%20Medical%20Centre%20CR%20Simon%20Maude.jpg?itok=Z6u9d0XH)
![Mary Toloa, specialist GP at Porirua and Union Community Health Service in Wellington, Mara Coler, clinical pharmacist at Tū Ora Compass Health, and Bhavna Mistry, specialist GP at Porirua and Union Community Health Service [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/9.%20Mary%20Toloa%2C%20Porirua%20and%20Union%20Community%20Health%20Service%20in%20Wellington%2C%20Mara%20Coler%2C%20T%C5%AB%20Ora%20Compass%20Health%2C%20and%20Bhavna%20Mistry%2C%20PUCHS%20CR%20Simon%20Maude.jpg?itok=kpChr0cc)