High cost rises and low government funding could see patient fee increases of up to 13.39 per cent allowed at some practices – the highest ever allowed under capitation funding.
However, in an emailed statement, Te Whatu Ora Living Well director Martin Hefford says that while the agency sets the maximum fee increase, general practices decide their fee increases, and the “actual fees vary considerably”.
Consultant Sapere, which has calculated the Annual Statement of Reasonable Fee Increases for nearly 20 years, says this year’s maximum fee increases “are the highest they have ever been”.
“This reflects the strong rises in input costs and the lower relative government funding contribution for this year,” Sapere says in its 2024/25 ASRFI report to Te Whatu Ora. The maximum fee increases range from 7.76 per cent for practices that receive 50 per cent of their income from capitation to 13.39 per cent for practices that rely on capitation for 80 per cent of their funding.
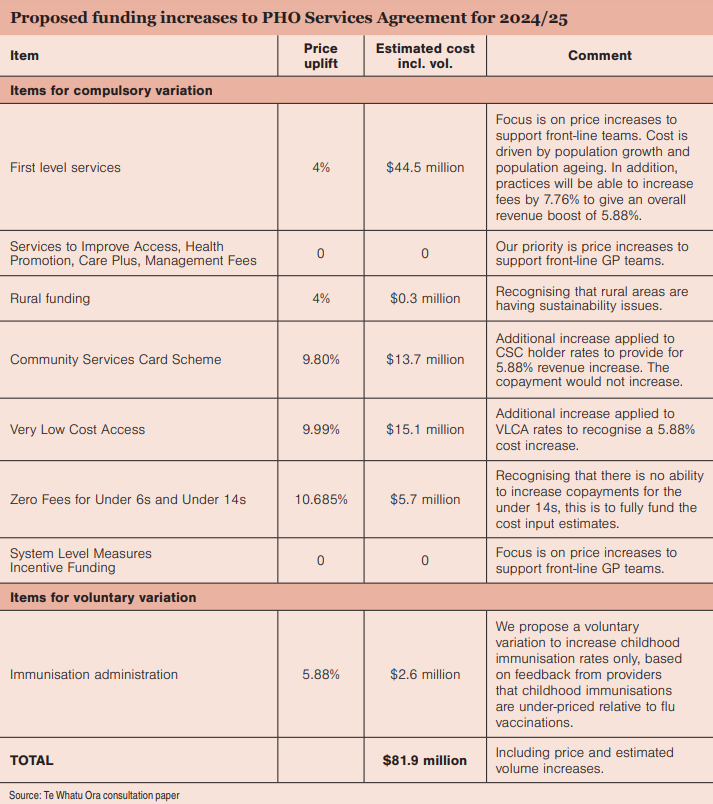
Te Whatu Ora acknowledges the “significant financial and workforce pressure” on general practice sustainability in its consultation paper to the sector on this year’s funding increase, Mr Hefford says. The increased offer considers the 5.88 per cent cost pressure figure, the need to stay within Budget 2024 appropriations, GP financial sustainability issues and the necessity to preserve primary care access for low-income New Zealanders.
With Very Low Cost Access practices in “many cases struggling financially”, the agency proposes a more significant funding increase to that sector. It is “open” to increasing patient fees for non-Community Services Card holders.
Also under consideration is a higher threshold for fee increases before practices had to apply to the Fees Review Committee, which will recognise the “financial issues” facing practices in general.
Possible relief for practices struggling to meet urgent and after-hours care obligations under the PHO Services Agreement due to “workforce constraints” is another proposal.
“Te Whatu Ora is open to considering the development of a protocol under which we would collaborate to address afterhours issues locally,” the consultation document says.
Primary care leaders refused to endorse an “inadequate” government funding offer that didn’t address “chronic underfunding”, an official communique confirms.
The communique, agreed to by members of the PHO Services Agreement Amendment Protocol, was released by Te Whatu Ora after the agency presented the 4 per cent capitation increase to the sector at the PSAAP forum on 19 June (see full offer details in panels).
PSAAP members “expressed significant concerns” at the offer’s “inadequacy” and the “highly unsatisfactory” compressed PSAAP process, which didn’t allow adequate time for negotiations or consultation.
“The overall feedback was that the financial sustainability of the sector is not advanced by this proposal,” the communique says, and “PHOs and contracted providers were unable to endorse the proposal”. The agency agreed to PSAAP members’ requests for a 20-day consultation period with a decision to be made on 20 July so payments could be made in August and back-dated to 1 July.


![NZ cash, money, notes [Thomas Coker on Unsplash]](/sites/default/files/styles/cropped_image_4_3/public/2024-05/thomas-coker-M8fYycGWuMA-unsplash.jpg?itok=0I2O_NFl)


![Tug of war money [Alashi on iStock]](/sites/default/files/styles/cropped_image_4_3/public/2024-03/Tug%20of%20war%20money%20and%20hand_CR_iStock-808110400_alashi.jpg?itok=zKaJClcm)





![Barbara Fountain, editor of New Zealand Doctor Rata Aotearoa, and Paul Hutchison, GP and senior medical clinician at Tāmaki Health [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/Barbara%20Fountain%2C%20editor%20of%20New%20Zealand%20Doctor%20Rata%20Aotearoa%2C%20and%20Paul%20Hutchison%2C%20GP%20and%20senior%20medical%20clinician%20at%20T%C4%81maki%20Health%20CR%20Simon%20Maude.jpg?itok=-HbQ1EYA)
![Lori Peters, NP and advanced health improvement practitioner at Mahitahi Hauora, and Jasper Nacilla, NP at The Terrace Medical Centre in Wellington [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/2.%20Lori%20Peters%2C%20NP%20and%20advanced%20HIP%20at%20Mahitahi%20Hauora%2C%20and%20Jasper%20Nacilla%2C%20NP%20at%20The%20Terrace%20Medical%20Centre%20in%20Wellington%20CR%20Simon%20Maude.jpg?itok=sUfbsSF1)
![Ministry of Social Development health and disability coordinator Liz Williams, regional health advisors Mary Mojel and Larah Takarangi, and health and disability coordinators Rebecca Staunton and Myint Than Htut [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/3.%20Ministry%20of%20Social%20Development%27s%20Liz%20Williams%2C%20Mary%20Mojel%2C%20Larah%20Takarangi%2C%20Rebecca%20Staunton%20and%20Myint%20Than%20Htut%20CR%20Simon%20Maude.jpg?itok=9ceOujzC)
![Locum GP Helen Fisher, with Te Kuiti Medical Centre NP Bridget Woodney [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/4.%20Locum%20GP%20Helen%20Fisher%2C%20with%20Te%20Kuiti%20Medical%20Centre%20NP%20Bridget%20Woodney%20CR%20Simon%20Maude.jpg?itok=TJeODetm)
![Ruby Faulkner, GPEP2, with David Small, GPEP3 from The Doctors Greenmeadows in Napier [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/5.%20Ruby%20Faulkner%2C%20GPEP2%2C%20with%20David%20Small%2C%20GPEP3%20from%20The%20Doctors%20Greenmeadows%20in%20Napier%20CR%20Simon%20Maude.jpg?itok=B0u4wsIs)
![Rochelle Langton and Libby Thomas, marketing advisors at the Medical Protection Society [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/6.%20Rochelle%20Langton%20and%20Libby%20Thomas%2C%20marketing%20advisors%20at%20the%20Medical%20Protection%20Society%20CR%20Simon%20Maude.jpg?itok=r52_Cf74)
![Specialist GP Lucy Gibberd, medical advisor at MPS, and Zara Bolam, urgent-care specialist at The Nest Health Centre in Inglewood [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/7.%20Specialist%20GP%20Lucy%20Gibberd%2C%20medical%20advisor%20at%20MPS%2C%20and%20Zara%20Bolam%2C%20urgent-care%20specialist%20at%20The%20Nest%20Health%20Centre%20in%20Inglewood%20CR%20Simon%20Maude.jpg?itok=z8eVoBU3)
![Olivia Blackmore and Trudee Sharp, NPs at Gore Health Centre, and Gaylene Hastie, NP at Queenstown Medical Centre [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/8.%20Olivia%20Blackmore%20and%20Trudee%20Sharp%2C%20NPs%20at%20Gore%20Health%20Centre%2C%20and%20Gaylene%20Hastie%2C%20NP%20at%20Queenstown%20Medical%20Centre%20CR%20Simon%20Maude.jpg?itok=Z6u9d0XH)
![Mary Toloa, specialist GP at Porirua and Union Community Health Service in Wellington, Mara Coler, clinical pharmacist at Tū Ora Compass Health, and Bhavna Mistry, specialist GP at Porirua and Union Community Health Service [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/9.%20Mary%20Toloa%2C%20Porirua%20and%20Union%20Community%20Health%20Service%20in%20Wellington%2C%20Mara%20Coler%2C%20T%C5%AB%20Ora%20Compass%20Health%2C%20and%20Bhavna%20Mistry%2C%20PUCHS%20CR%20Simon%20Maude.jpg?itok=kpChr0cc)