Zoledronate infusion has the advantage that it only needs to be administered every 18 to 24 months, resulting in better patient acceptance and adherence
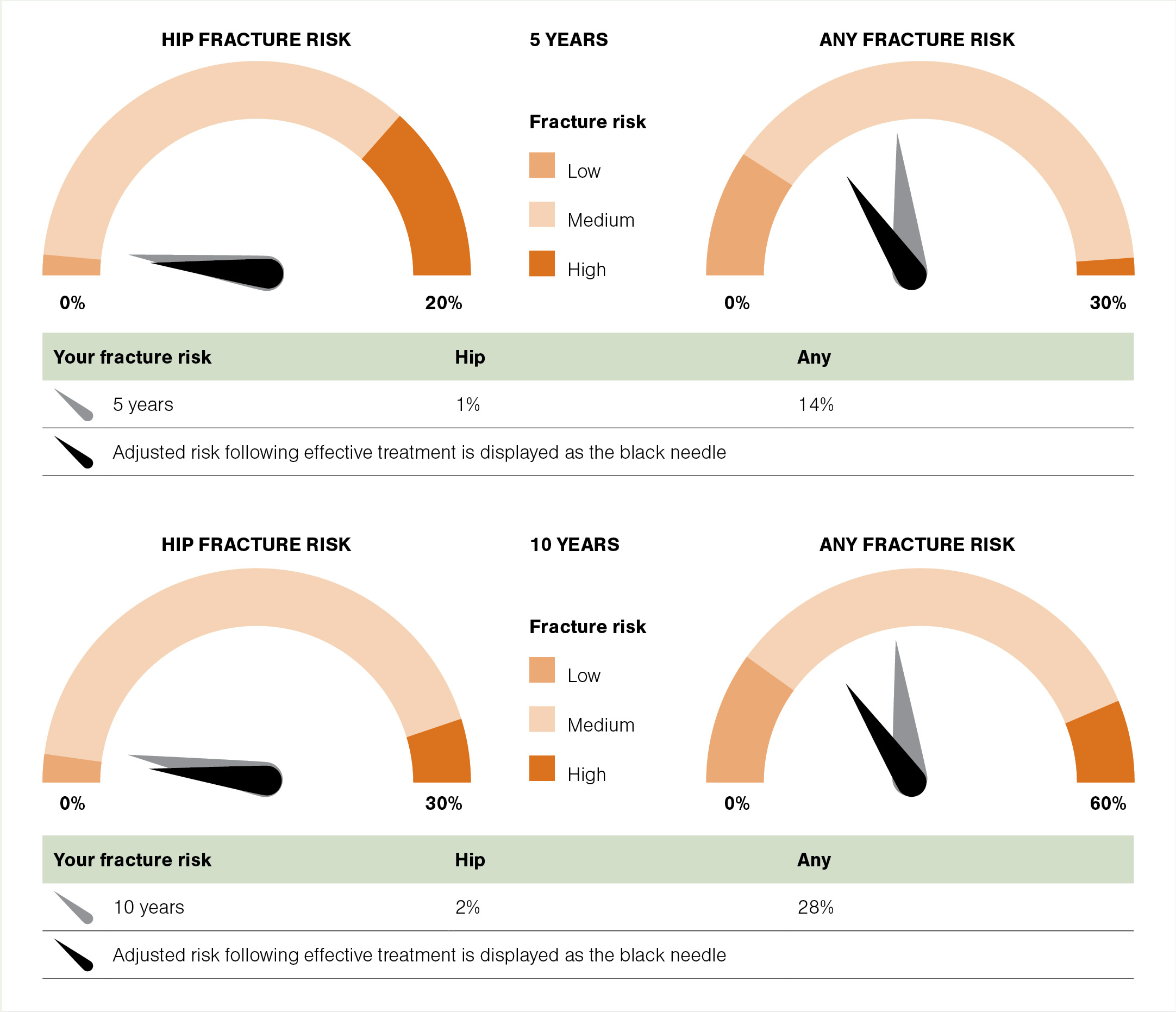
Regardless of whether there has been a fragility fracture or not, those at sufficiently high risk of future fractures should be considered for pharmacotherapy (a 10-year hip fracture risk above 3 per cent, using the FRAX or Garvan calculators, is often used as the threshold). This would include the majority of those having had any fragility fracture, especially those over age 75. This is the reason why a DXA scan is generally not necessary prior to initiating anti-osteoporosis treatment in this cohort. In particular, those with vertebral or hip fractures (associated with the highest risk of further fractures) should have lower threshold for treatment initiation after the sentinel fracture.
In the absence of fracture, treatment is also generally indicated in those whose DXA T-score is less than or equal to -2.5, or less than or equal to -1.5 with significant risk factors such that their fracture risk is high.
Oral and intravenous bisphosphonates
Bisphosphonates remain the first line and mainstay of anti-osteoporosis treatment, both locally and internationally. The ANZFFR Annual Report 2024 shows 95 per cent of anti-osteoporosis treatment used is either oral or intravenous bisphosphonate. Oral agents available in New Zealand are alendronate (Fosamax and Fosamax Plus) and risedronate, and the intravenous agent for use in osteoporosis is zoledronate. In the past, alendronate and zoledronate were funded under Special Authority restrictions, but both are now fully funded without restriction.
Studies suggest poor adherence to oral bisphosphonates. Therefore, it is recommended that adherence is checked periodically and that a blood test for procollagen-1 N-terminal peptide (P1NP) is performed about six months after starting treatment. P1NP is a bone formation (and hence turnover) marker that is suppressed (below 35µg/L) when oral bisphosphonate is taken regularly and absorbed adequately. Switching to intravenous zoledronate should be considered if P1NP is above 35µg/L despite seemingly good adherence or where consistent adherence is problematic.
Zoledronate infusion has the advantage that it only needs to be administered every 18 to 24 months, resulting in better patient acceptance and adherence. It can be used in patients who experienced side effects from, or have contraindications to, oral bisphosphonates.
A very common adverse effect of zoledronate infusion is post-dose flu-like symptoms that occur in up to one-third of patients after the first dose. This acute-phase response typically occurs in the first few days of drug infusion and resolves within three days or so. Paracetamol with or without an NSAID can be used to alleviate symptoms (the latter only if safe to use for the individual patient and deemed necessary). Incidence of this post-infusion adverse effect markedly decreases with subsequent infusions.
A recent New Zealand study showed that a three-day course of oral dexamethasone (4mg daily, started on the day of infusion) significantly reduced the acute-phase response (J Bone Miner Res 2023;38[5]:631–38). This approach could be considered either routinely or in those with significant prior post-infusion acute-phase response.
With the recent funding change for zoledronate, the fully funded product is no longer the well-known Aclasta but the generic version Zoledronic Acid Viatris. Therefore, we should avoid prescribing it as Aclasta, but instead prescribe zoledronate or zoledronic acid.
There remains an access inequality issue due to the zoledronate infusion fee that is charged by private and primary care providers. Due to the sheer volume of patients treated with zoledronate, secondary care in most regions of New Zealand is unable to offer infusions for all. There is an ongoing push by Osteoporosis New Zealand and Fracture Liaison Network New Zealand towards equitable and improved access for zoledronate infusions nationally.
Contraindications and adverse effects
Contraindications to bisphosphonates include renal failure – denoted in Medsafe data sheets as creatinine clearance (CrCl) <35ml/min for zoledronate and oral bisphosphonates. It is common practice to reduce the administration dose of zoledronate (eg, from 5mg to 2.5mg) and/or slow the infusion rate (over 30 to 60 minutes) when treating patients with a lower CrCl of 35–50ml/min.
Use of zoledronate in those with lower renal functions (eg, CrCl 25–35ml/min) and use of estimated glomerular filtration rate instead of CrCl remain controversial. Lower renal function threshold – possibly CrCl down to 15ml/min – for oral bisphosphonates is believed to be safe. Evidence for safety of this off-label use for oral bisphosphonates in stage 4 chronic kidney disease is scant, and hopefully will not be necessary once the access of denosumab (discussed in the next section) improves.
Oral bisphosphonates should also be avoided in those with significant impairment or delay in oesophageal emptying, such as oesophageal stricture or achalasia.
A well-publicised side effect of bisphosphonates is osteonecrosis of the jaw (ONJ). It manifests as an area of exposed bone in the mouth that does not heal within eight weeks. In reality, it is extremely rare in the setting of osteoporosis management. It is, nevertheless, recommended that significant dental issues requiring major dental work (eg, dental implants, multiple teeth extractions or jaw surgery) are resolved before initiation of bisphosphonate therapy.
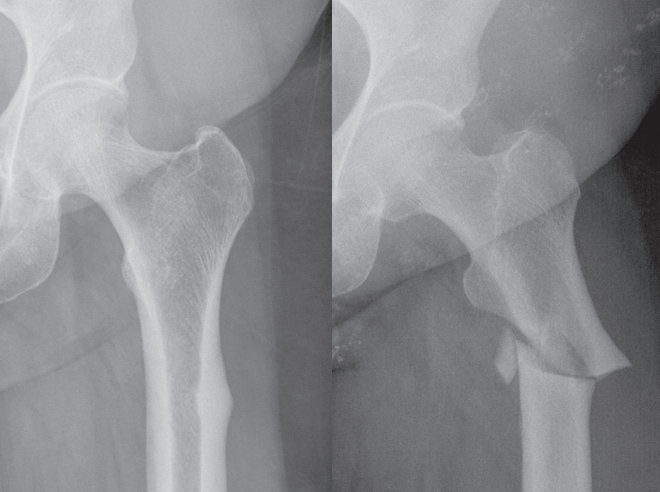
Another bisphosphonate-related long-term adverse effect is that of atypical femoral fracture (AFF). These initially begin as stress fractures in the lateral cortex of the femoral shaft and can spontaneously progress to full-thickness transverse fractures of the femur. Before fracture, the lateral cortex of the femur may appear thickened on x-ray, with a “beaked” appearance (Figure 3).
The incidence of AFF, albeit very low in absolute risk terms (several cases per 100,000 person-years), appears to increase steeply with increasing duration of bisphosphonate use, largely with oral forms, beyond five to seven years of treatment, and risk drops off dramatically within one to two years of treatment intermission or cessation. Thus, it is important to periodically review the need for continued bisphosphonate therapy and provide “drug holidays” (discussed below) for patients requiring therapy for more than five years.











![Barbara Fountain, editor of New Zealand Doctor Rata Aotearoa, and Paul Hutchison, GP and senior medical clinician at Tāmaki Health [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/Barbara%20Fountain%2C%20editor%20of%20New%20Zealand%20Doctor%20Rata%20Aotearoa%2C%20and%20Paul%20Hutchison%2C%20GP%20and%20senior%20medical%20clinician%20at%20T%C4%81maki%20Health%20CR%20Simon%20Maude.jpg?itok=-HbQ1EYA)
![Lori Peters, NP and advanced health improvement practitioner at Mahitahi Hauora, and Jasper Nacilla, NP at The Terrace Medical Centre in Wellington [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/2.%20Lori%20Peters%2C%20NP%20and%20advanced%20HIP%20at%20Mahitahi%20Hauora%2C%20and%20Jasper%20Nacilla%2C%20NP%20at%20The%20Terrace%20Medical%20Centre%20in%20Wellington%20CR%20Simon%20Maude.jpg?itok=sUfbsSF1)
![Ministry of Social Development health and disability coordinator Liz Williams, regional health advisors Mary Mojel and Larah Takarangi, and health and disability coordinators Rebecca Staunton and Myint Than Htut [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/3.%20Ministry%20of%20Social%20Development%27s%20Liz%20Williams%2C%20Mary%20Mojel%2C%20Larah%20Takarangi%2C%20Rebecca%20Staunton%20and%20Myint%20Than%20Htut%20CR%20Simon%20Maude.jpg?itok=9ceOujzC)
![Locum GP Helen Fisher, with Te Kuiti Medical Centre NP Bridget Woodney [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/4.%20Locum%20GP%20Helen%20Fisher%2C%20with%20Te%20Kuiti%20Medical%20Centre%20NP%20Bridget%20Woodney%20CR%20Simon%20Maude.jpg?itok=TJeODetm)
![Ruby Faulkner, GPEP2, with David Small, GPEP3 from The Doctors Greenmeadows in Napier [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/5.%20Ruby%20Faulkner%2C%20GPEP2%2C%20with%20David%20Small%2C%20GPEP3%20from%20The%20Doctors%20Greenmeadows%20in%20Napier%20CR%20Simon%20Maude.jpg?itok=B0u4wsIs)
![Rochelle Langton and Libby Thomas, marketing advisors at the Medical Protection Society [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/6.%20Rochelle%20Langton%20and%20Libby%20Thomas%2C%20marketing%20advisors%20at%20the%20Medical%20Protection%20Society%20CR%20Simon%20Maude.jpg?itok=r52_Cf74)
![Specialist GP Lucy Gibberd, medical advisor at MPS, and Zara Bolam, urgent-care specialist at The Nest Health Centre in Inglewood [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/7.%20Specialist%20GP%20Lucy%20Gibberd%2C%20medical%20advisor%20at%20MPS%2C%20and%20Zara%20Bolam%2C%20urgent-care%20specialist%20at%20The%20Nest%20Health%20Centre%20in%20Inglewood%20CR%20Simon%20Maude.jpg?itok=z8eVoBU3)
![Olivia Blackmore and Trudee Sharp, NPs at Gore Health Centre, and Gaylene Hastie, NP at Queenstown Medical Centre [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/8.%20Olivia%20Blackmore%20and%20Trudee%20Sharp%2C%20NPs%20at%20Gore%20Health%20Centre%2C%20and%20Gaylene%20Hastie%2C%20NP%20at%20Queenstown%20Medical%20Centre%20CR%20Simon%20Maude.jpg?itok=Z6u9d0XH)
![Mary Toloa, specialist GP at Porirua and Union Community Health Service in Wellington, Mara Coler, clinical pharmacist at Tū Ora Compass Health, and Bhavna Mistry, specialist GP at Porirua and Union Community Health Service [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/9.%20Mary%20Toloa%2C%20Porirua%20and%20Union%20Community%20Health%20Service%20in%20Wellington%2C%20Mara%20Coler%2C%20T%C5%AB%20Ora%20Compass%20Health%2C%20and%20Bhavna%20Mistry%2C%20PUCHS%20CR%20Simon%20Maude.jpg?itok=kpChr0cc)