1.1: Prevention and early detection of melanoma
As melanoma in New Zealand is predominantly due to ultraviolet radiation, we need to raise awareness of the damage done by solar exposure and tanning devices in all skin types and ethnicities. Exposure to UV radiation should be limited and sunburn avoided.
The danger of UV radiation is reported as the UV Index. If it is over 3 (September to April), people should be advised to limit time outdoors, choose shade, protect their eyes with wrap-around sunglasses, and protect their skin with long sleeves, a collar and a wide-brimmed hat. Broad-spectrum and water-resistant sunscreen with a sun protection factor of at least 50 should be reapplied every two hours while outdoors during the day.
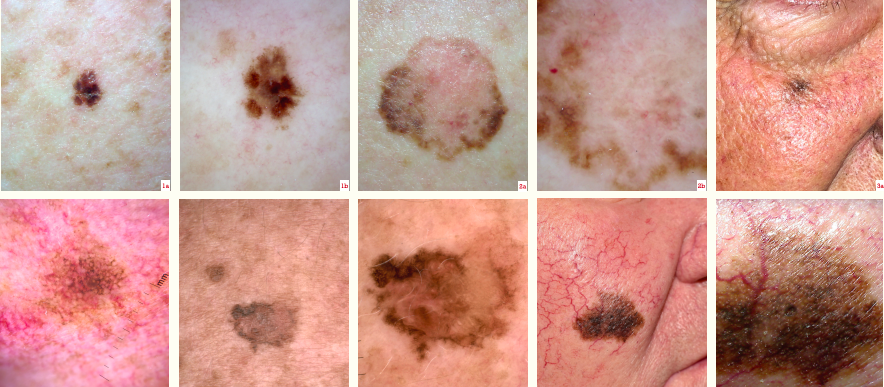
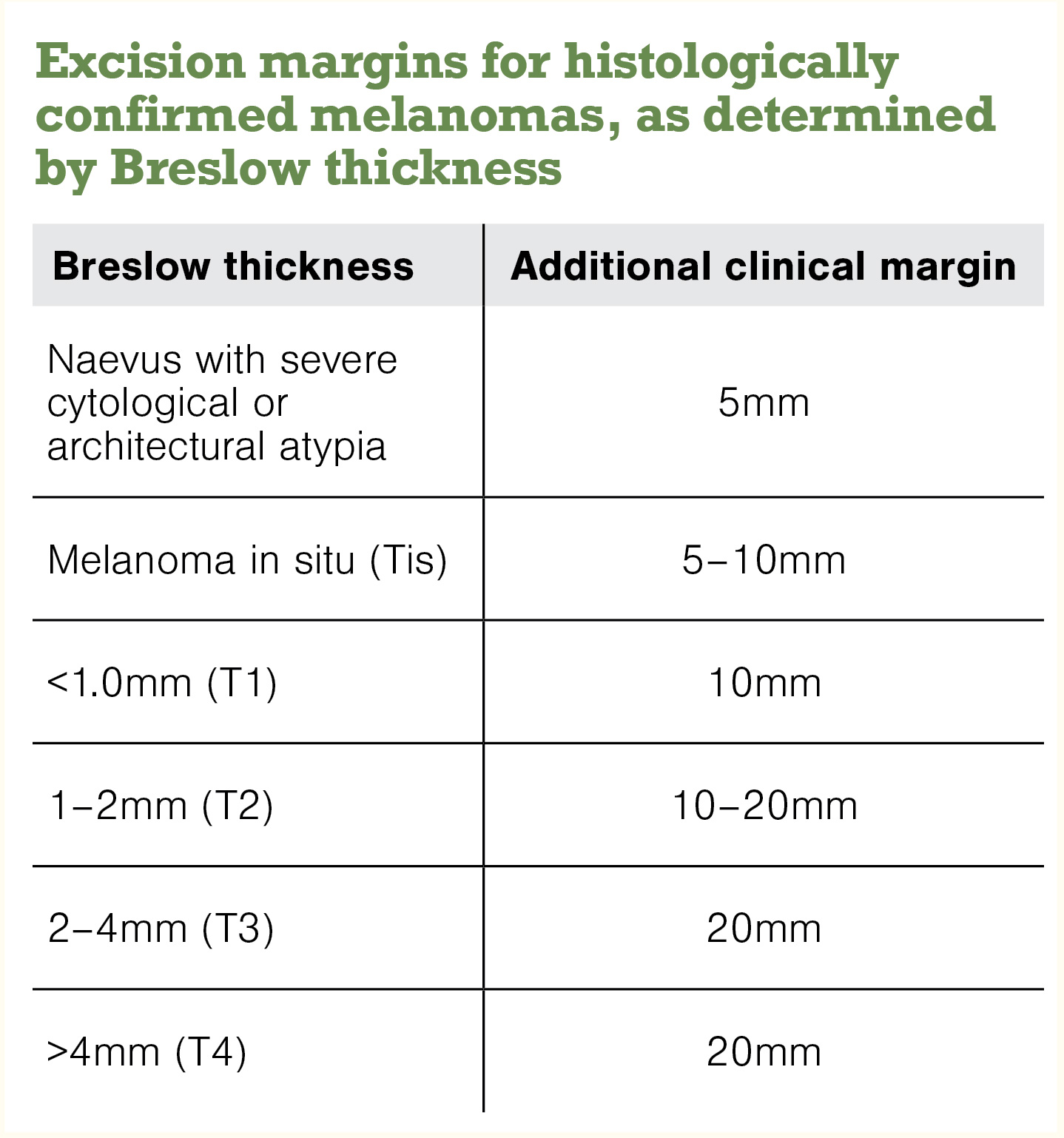
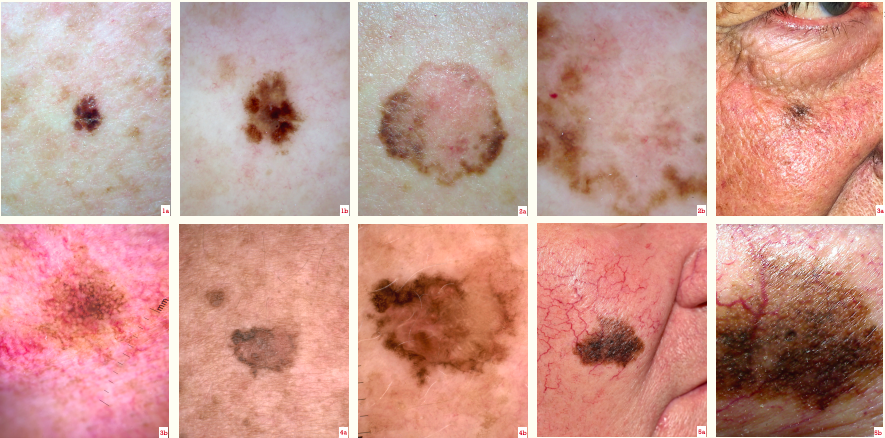
Although dark skin is less prone to melanoma, Māori and other ethnic minorities are likely to be diagnosed with thicker melanoma with poorer survival than non-Māori. Early detection reduces the chance of a poor outcome; long-term survival depends on the thickness of the melanoma at the time of excision. Many forms of melanoma can be identified when in situ (non-invasive).
Encourage your adult patients – especially those over age 50 – to examine their own skin (with the help of a partner) and to seek advice from a health professional about any suspicious lesion. Explain they should expect a full-body skin check using dermatoscopy.
1.2: Training of primary healthcare professionals
Most melanomas are spotted or confirmed in primary care; thus, it is essential that primary care professionals have the competence to diagnose them and know what to do. In 2022, patients with melanoma can expect their examination to include dermatoscopy. The fundamental skills should be included as part of the General Practice Education Programme.
If you care for patients with melanoma or you undertake skin checks, the good practice points for quality statement 1.2 expect you to:
- know how to assess the patient’s risk of melanoma
- be alert for lesions with malignant features (and become familiar with the appearance of benign keratoses and melanocytic naevi – refer back to “Dermatology”, New Zealand Doctor, 12 May and 1 September 2021)
- be trained in the basic use of a dermatoscope and to refresh your knowledge
- arrange a full-body skin check for a patient at risk or presenting with a lesion of concern.
1.3: People at increased risk of melanoma
Anyone can get melanoma – most adults are at average risk and children and very dark-skinned individuals are at lower risk. It’s useful to identify people at higher risk to encourage them to present early with concerns about a skin lesion and schedule skin checks at appropriate intervals.
The usual reasons for high risk are increased age, fair skin and sun damage. Individuals may also have had a previous melanoma, familial melanoma (rare), many melanocytic naevi, giant congenital naevus, previous keratinocyte cancer or immunosuppression (especially organ transplant recipients).
A validated model for individuals to assess their risk of melanoma is provided by the Melanoma Institute Australia (melanomarisk.org.au). New Zealanders should enter Tasmania as the “Region of Australia most lived in”
People who have had melanoma, two or more first-degree relatives who had melanoma before they were 40, or many moles (especially if these are atypical) should be under the long-term care of a healthcare professional who is competent in skin surveillance using dermatoscopy and digital dermatoscopy. Consider baseline total-body photography and high-quality sequential digital dermatoscopy imaging annually for these patients.






![Barbara Fountain, editor of New Zealand Doctor Rata Aotearoa, and Paul Hutchison, GP and senior medical clinician at Tāmaki Health [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/Barbara%20Fountain%2C%20editor%20of%20New%20Zealand%20Doctor%20Rata%20Aotearoa%2C%20and%20Paul%20Hutchison%2C%20GP%20and%20senior%20medical%20clinician%20at%20T%C4%81maki%20Health%20CR%20Simon%20Maude.jpg?itok=-HbQ1EYA)
![Lori Peters, NP and advanced health improvement practitioner at Mahitahi Hauora, and Jasper Nacilla, NP at The Terrace Medical Centre in Wellington [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/2.%20Lori%20Peters%2C%20NP%20and%20advanced%20HIP%20at%20Mahitahi%20Hauora%2C%20and%20Jasper%20Nacilla%2C%20NP%20at%20The%20Terrace%20Medical%20Centre%20in%20Wellington%20CR%20Simon%20Maude.jpg?itok=sUfbsSF1)
![Ministry of Social Development health and disability coordinator Liz Williams, regional health advisors Mary Mojel and Larah Takarangi, and health and disability coordinators Rebecca Staunton and Myint Than Htut [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/3.%20Ministry%20of%20Social%20Development%27s%20Liz%20Williams%2C%20Mary%20Mojel%2C%20Larah%20Takarangi%2C%20Rebecca%20Staunton%20and%20Myint%20Than%20Htut%20CR%20Simon%20Maude.jpg?itok=9ceOujzC)
![Locum GP Helen Fisher, with Te Kuiti Medical Centre NP Bridget Woodney [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/4.%20Locum%20GP%20Helen%20Fisher%2C%20with%20Te%20Kuiti%20Medical%20Centre%20NP%20Bridget%20Woodney%20CR%20Simon%20Maude.jpg?itok=TJeODetm)
![Ruby Faulkner, GPEP2, with David Small, GPEP3 from The Doctors Greenmeadows in Napier [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/5.%20Ruby%20Faulkner%2C%20GPEP2%2C%20with%20David%20Small%2C%20GPEP3%20from%20The%20Doctors%20Greenmeadows%20in%20Napier%20CR%20Simon%20Maude.jpg?itok=B0u4wsIs)
![Rochelle Langton and Libby Thomas, marketing advisors at the Medical Protection Society [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/6.%20Rochelle%20Langton%20and%20Libby%20Thomas%2C%20marketing%20advisors%20at%20the%20Medical%20Protection%20Society%20CR%20Simon%20Maude.jpg?itok=r52_Cf74)
![Specialist GP Lucy Gibberd, medical advisor at MPS, and Zara Bolam, urgent-care specialist at The Nest Health Centre in Inglewood [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/7.%20Specialist%20GP%20Lucy%20Gibberd%2C%20medical%20advisor%20at%20MPS%2C%20and%20Zara%20Bolam%2C%20urgent-care%20specialist%20at%20The%20Nest%20Health%20Centre%20in%20Inglewood%20CR%20Simon%20Maude.jpg?itok=z8eVoBU3)
![Olivia Blackmore and Trudee Sharp, NPs at Gore Health Centre, and Gaylene Hastie, NP at Queenstown Medical Centre [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/8.%20Olivia%20Blackmore%20and%20Trudee%20Sharp%2C%20NPs%20at%20Gore%20Health%20Centre%2C%20and%20Gaylene%20Hastie%2C%20NP%20at%20Queenstown%20Medical%20Centre%20CR%20Simon%20Maude.jpg?itok=Z6u9d0XH)
![Mary Toloa, specialist GP at Porirua and Union Community Health Service in Wellington, Mara Coler, clinical pharmacist at Tū Ora Compass Health, and Bhavna Mistry, specialist GP at Porirua and Union Community Health Service [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/9.%20Mary%20Toloa%2C%20Porirua%20and%20Union%20Community%20Health%20Service%20in%20Wellington%2C%20Mara%20Coler%2C%20T%C5%AB%20Ora%20Compass%20Health%2C%20and%20Bhavna%20Mistry%2C%20PUCHS%20CR%20Simon%20Maude.jpg?itok=kpChr0cc)