For the secondary prevention of vascular disease…there are two options for funding
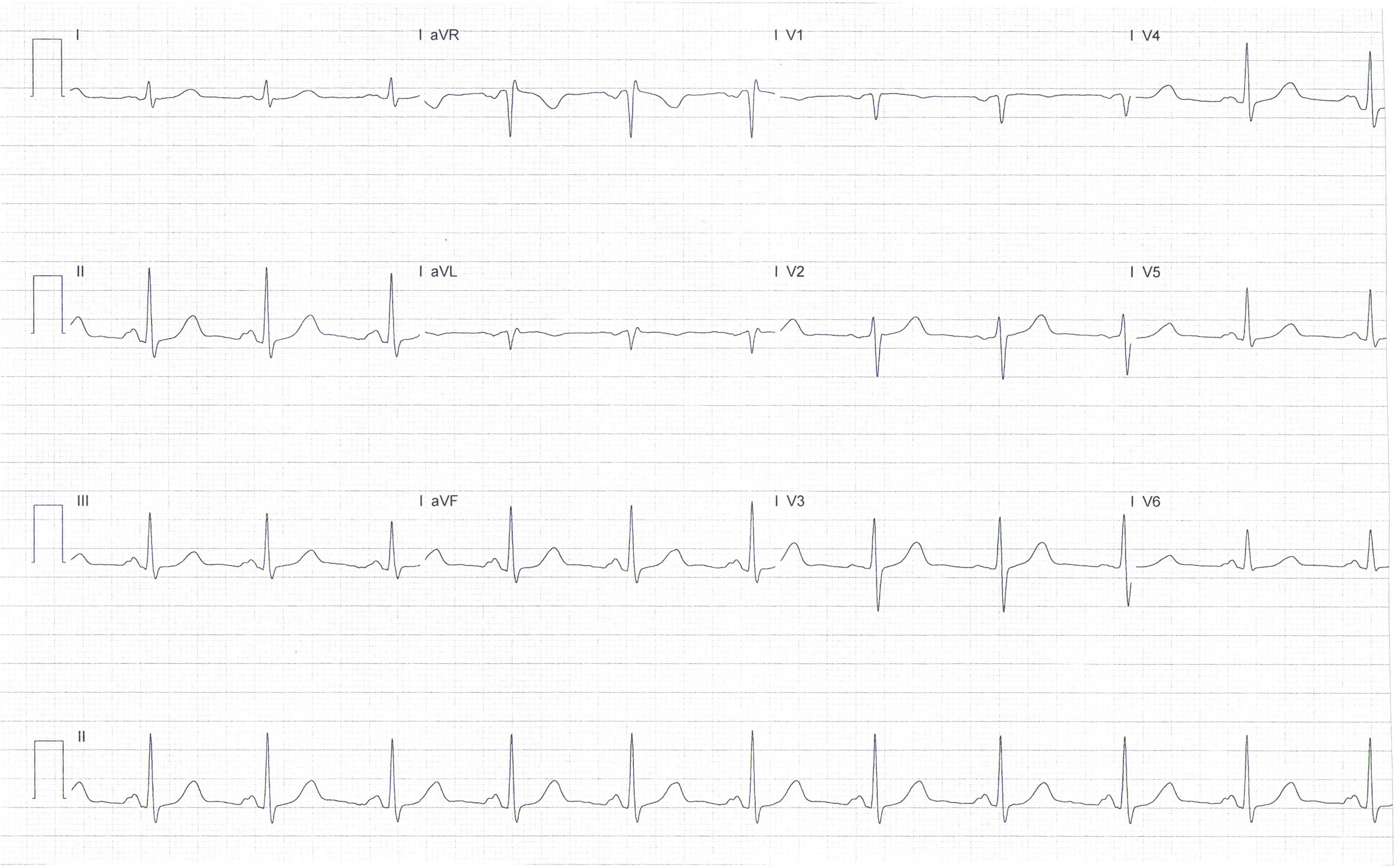
1. The ECG shows sinus rhythm, a normal axis and a rate of 72 beats per minute. It is within normal limits. This is often the situation after a non-STEMI presentation.
2. In 2005, rosuvastatin was not funded when first considered by Pharmac, but it was still fairly widely used by patients who could pay for it, at about $60 per month. Many patients find rosuvastatin causes less myalgia, possibly due to it being hydrophilic, with less tissue absorption and, hence, fewer adverse effects than the lipophilic atorvastatin.
Now, some 16 years later, from 1 December 2021, Pharmac has designed Special Authority criteria to fund rosuvastatin. Arguably, the most important feature of this change has been the recognition that a lower LDL cholesterol target should be achieved in New Zealand patients than has previously been funded by Pharmac.
For the primary prevention of vascular disease, there are two options for funding of patients: some patients with “cardiovascular disease risk” (defined) and some patients with “familial hypercholesterolaemia” (defined) are now eligible. Discussion of this is outside the scope of this article.
For the secondary prevention of vascular disease, such as your patient, there are also two options for funding:
- The first option is for patients with “established cardiovascular disease”, which is defined as one of three groups – patients with proven coronary artery disease, proven peripheral artery disease, or who have experienced an ischaemic stroke. However, in addition, patients must have an LDL cholesterol which “has not reduced to less than 1.4mmol/L with treatment with the maximum tolerated dose of atorvastatin and/or simvastatin”.
- The second option is for patients who have experienced “recurrent major cardiovascular events”, which is defined as one of four groups: myocardial infarction, ischaemic stroke, coronary revascularisation or hospitalisation for unstable angina in the last two years. In addition, patients must have an LDL cholesterol which “has not reduced to less than 1.0mmol/L with treatment with the maximum tolerated dose of atorvastatin and/or simvastatin”.
3. With the funding of rosuvastatin, there is a recognition that patients will benefit from lower LDL cholesterol levels than were previously funded. In fact, it has been known for many years that lowering LDL cholesterol reduces the risk of atherosclerotic cardiovascular disease proportional to the reduction in LDL cholesterol.
Reduction in LDL cholesterol can be achieved with several medicines: statins and ezetimibe, bile-acid resins and fibrates (both rarely used and of limited benefit), as well as newer agents, such as bempedoic acid (not available or funded in New Zealand) or the PCSK9 inhibitors (eg, alirocumab, which is available but not funded in New Zealand).
The new Special Authority form accepts the funding of an LDL cholesterol target of <1.4mmol/L for all patients with established vascular disease, and an LDL cholesterol target of <1.0mmol/L for those at the very highest risk, with a recurrent vascular event within two years of the prior event.
4. Your patient now qualifies for a change from atorvastatin to rosuvastatin. The highest rosuvastatin dose (40mg) should lower the LDL cholesterol level by approximately 63 per cent, which is an extra 8 per cent compared with the top atorvastatin dose (80mg), which will lower the LDL cholesterol level by about 55 per cent.
5. His LDL cholesterol is now 1.7mmol/L. Unfortunately, he does not qualify for funding for the addition of ezetimibe, which would further lower the LDL cholesterol by approximately 20 per cent. For ezetimibe funding, Pharmac requires the LDL cholesterol level to be ≥2mmol/L on the highest tolerated dose of atorvastatin. Some patients now pay for ezetimibe treatment at about $45 dollars per month. However, your patient is unable to afford this.
6. The 2019 European guidelines for the management of dyslipidaemias set these vigorous targets,1 which are now used by Pharmac. This is a very significant, and welcome, change in approach for New Zealand patients.






![Barbara Fountain, editor of New Zealand Doctor Rata Aotearoa, and Paul Hutchison, GP and senior medical clinician at Tāmaki Health [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/Barbara%20Fountain%2C%20editor%20of%20New%20Zealand%20Doctor%20Rata%20Aotearoa%2C%20and%20Paul%20Hutchison%2C%20GP%20and%20senior%20medical%20clinician%20at%20T%C4%81maki%20Health%20CR%20Simon%20Maude.jpg?itok=-HbQ1EYA)
![Lori Peters, NP and advanced health improvement practitioner at Mahitahi Hauora, and Jasper Nacilla, NP at The Terrace Medical Centre in Wellington [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/2.%20Lori%20Peters%2C%20NP%20and%20advanced%20HIP%20at%20Mahitahi%20Hauora%2C%20and%20Jasper%20Nacilla%2C%20NP%20at%20The%20Terrace%20Medical%20Centre%20in%20Wellington%20CR%20Simon%20Maude.jpg?itok=sUfbsSF1)
![Ministry of Social Development health and disability coordinator Liz Williams, regional health advisors Mary Mojel and Larah Takarangi, and health and disability coordinators Rebecca Staunton and Myint Than Htut [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/3.%20Ministry%20of%20Social%20Development%27s%20Liz%20Williams%2C%20Mary%20Mojel%2C%20Larah%20Takarangi%2C%20Rebecca%20Staunton%20and%20Myint%20Than%20Htut%20CR%20Simon%20Maude.jpg?itok=9ceOujzC)
![Locum GP Helen Fisher, with Te Kuiti Medical Centre NP Bridget Woodney [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/4.%20Locum%20GP%20Helen%20Fisher%2C%20with%20Te%20Kuiti%20Medical%20Centre%20NP%20Bridget%20Woodney%20CR%20Simon%20Maude.jpg?itok=TJeODetm)
![Ruby Faulkner, GPEP2, with David Small, GPEP3 from The Doctors Greenmeadows in Napier [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/5.%20Ruby%20Faulkner%2C%20GPEP2%2C%20with%20David%20Small%2C%20GPEP3%20from%20The%20Doctors%20Greenmeadows%20in%20Napier%20CR%20Simon%20Maude.jpg?itok=B0u4wsIs)
![Rochelle Langton and Libby Thomas, marketing advisors at the Medical Protection Society [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/6.%20Rochelle%20Langton%20and%20Libby%20Thomas%2C%20marketing%20advisors%20at%20the%20Medical%20Protection%20Society%20CR%20Simon%20Maude.jpg?itok=r52_Cf74)
![Specialist GP Lucy Gibberd, medical advisor at MPS, and Zara Bolam, urgent-care specialist at The Nest Health Centre in Inglewood [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/7.%20Specialist%20GP%20Lucy%20Gibberd%2C%20medical%20advisor%20at%20MPS%2C%20and%20Zara%20Bolam%2C%20urgent-care%20specialist%20at%20The%20Nest%20Health%20Centre%20in%20Inglewood%20CR%20Simon%20Maude.jpg?itok=z8eVoBU3)
![Olivia Blackmore and Trudee Sharp, NPs at Gore Health Centre, and Gaylene Hastie, NP at Queenstown Medical Centre [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/8.%20Olivia%20Blackmore%20and%20Trudee%20Sharp%2C%20NPs%20at%20Gore%20Health%20Centre%2C%20and%20Gaylene%20Hastie%2C%20NP%20at%20Queenstown%20Medical%20Centre%20CR%20Simon%20Maude.jpg?itok=Z6u9d0XH)
![Mary Toloa, specialist GP at Porirua and Union Community Health Service in Wellington, Mara Coler, clinical pharmacist at Tū Ora Compass Health, and Bhavna Mistry, specialist GP at Porirua and Union Community Health Service [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/9.%20Mary%20Toloa%2C%20Porirua%20and%20Union%20Community%20Health%20Service%20in%20Wellington%2C%20Mara%20Coler%2C%20T%C5%AB%20Ora%20Compass%20Health%2C%20and%20Bhavna%20Mistry%2C%20PUCHS%20CR%20Simon%20Maude.jpg?itok=kpChr0cc)