Although effective, particularly for people at high risk of hospitalisation with COVID-19, care is required with nirmatrelvir/ritonavir because of the ritonavir component. Inhibition of the CYP3A4 enzyme system, to prevent rapid inactivation of the nirmatrelvir, means that it can also inhibit the metabolism of other medicines predominantly metabolised by CYP3A4, of which there are many.
A straightforward website provided by the University of Liverpool (covid19-druginteractions.org) enables rapid identification of potential interactions and includes a three-page colour chart for printing. For many interacting medicines, a one-week discontinuation (eg, statin) or dose reduction (eg, risperidone) is unlikely to have a large clinical impact.
Experience with the hepatitis C virus and HIV has raised awareness of the risk of viral resistance to monotherapy with antivirals. Nirmatrelvir/ritonavir is relatively new, and there is ongoing monitoring of resistance, with no significant concerns as yet.
There have been reports of viral load rebound a median of nine days after treatment in approximately 1 per cent of people. However, this does not appear to be associated with recurrence of severe disease or mutations.4,5
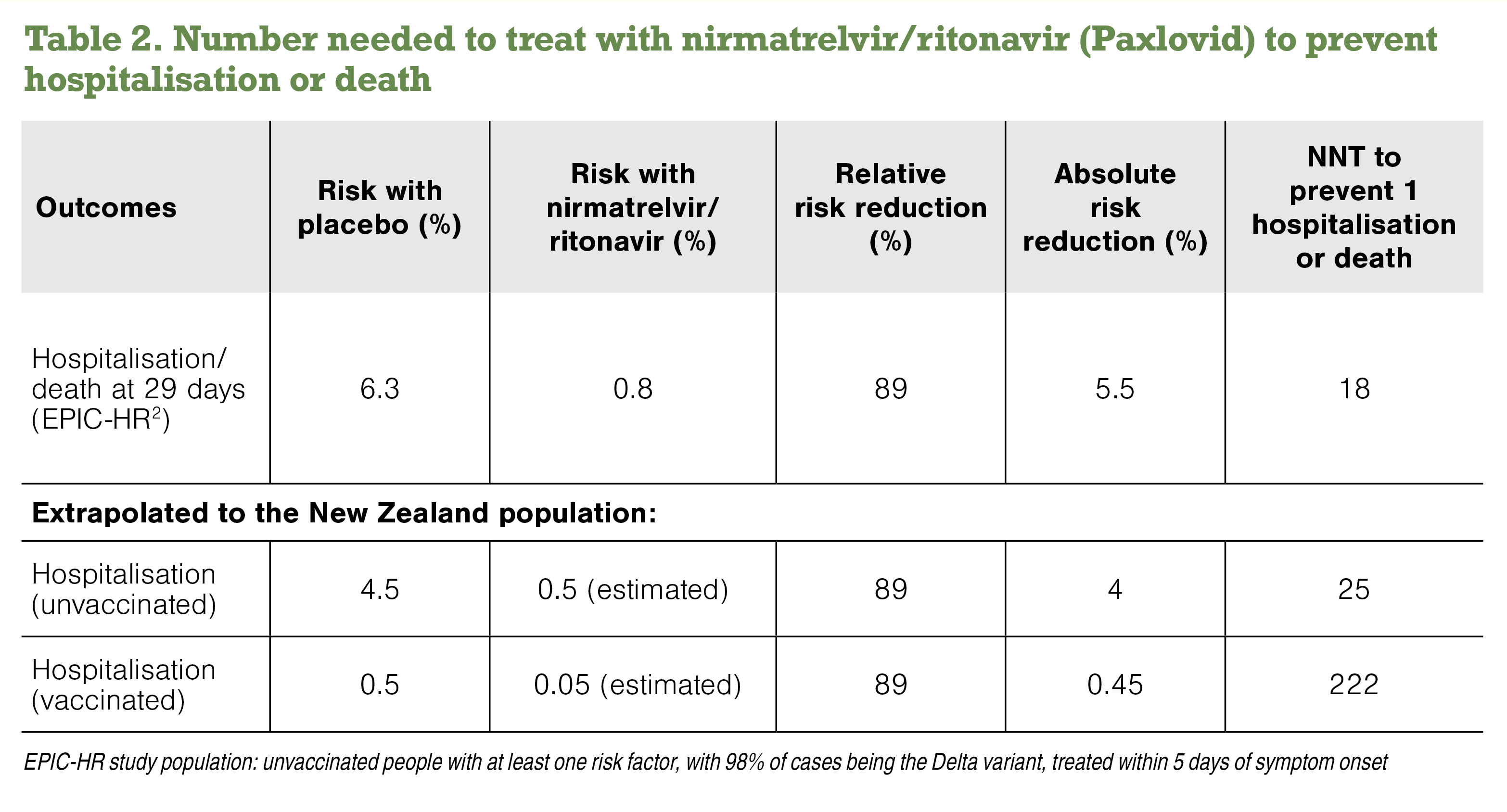
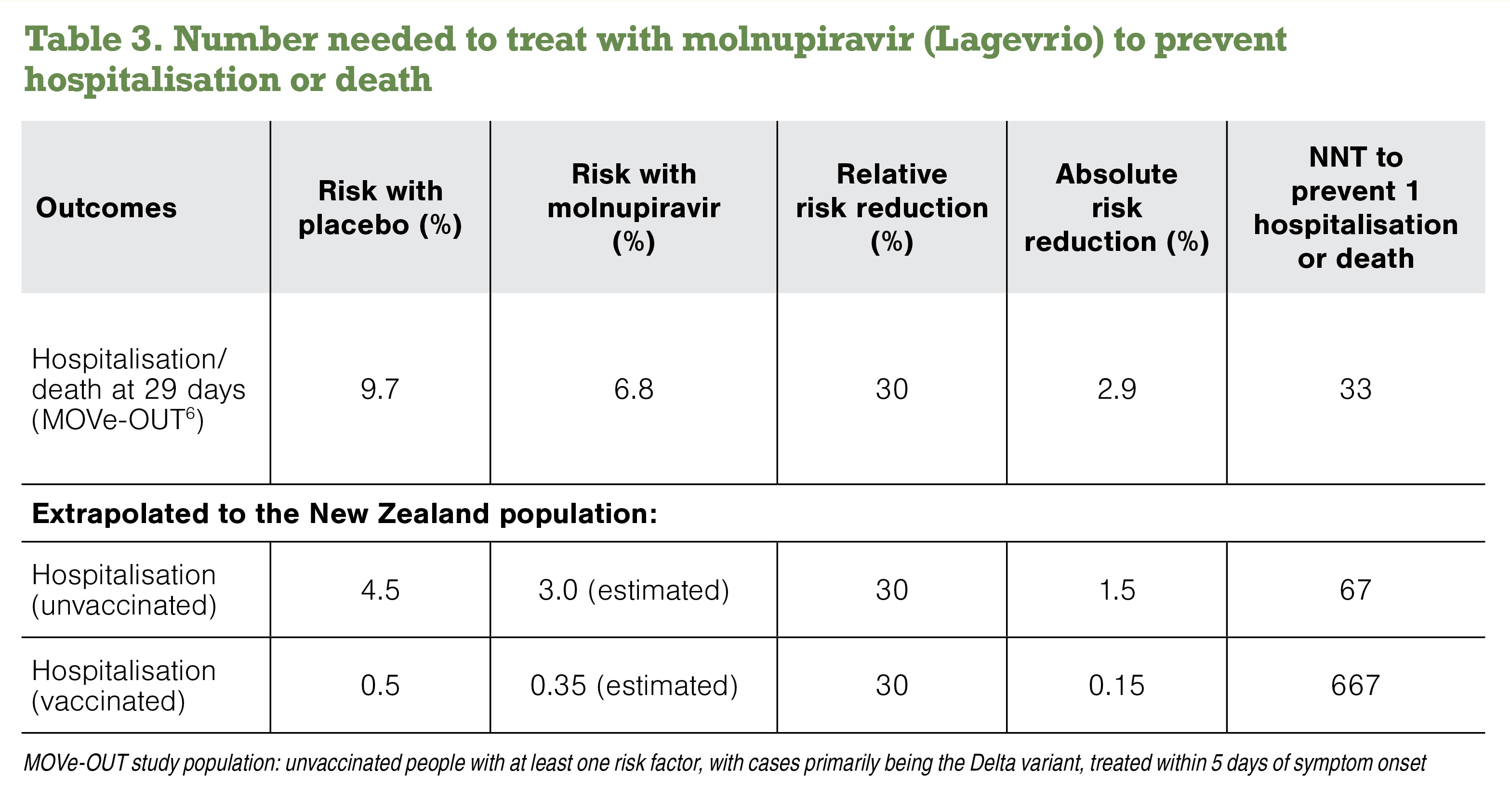
The principles of antimicrobial stewardship mean that nirmatrelvir/ritonavir should be used for those at risk of COVID-19 hospitalisation and not for low-risk people.
With renal dysfunction, nirmatrelvir/ritonavir is contraindicated at an estimated glomerular filtration rate of <30ml/min, and the dose should be reduced to one of each tablet twice daily at an eGFR of ≥30 to <60ml/min.
Note that the daily blister card contains two parts, each containing two tablets of nirmatrelvir and one tablet of ritonavir. People need to know which one to stop. They can take the unused nirmatrelvir back to the pharmacy but should not put them into a waterway (eg, down the sink).