He had stoically carried on at work despite being frightened he might “bring the virus home” to his family
A 55-year-old friend and colleague – an experienced physician at your local hospital – presents to you complaining of an increasing tendency to intermittently feel very short of breath during the daytime.
These episodes often occur in his office after his “morning” ward round, which currently takes five to seven hours to complete, when previously it was four hours on a busy day.
He explains that the delays are, in part, due to the personal protective equipment (PPE) he has to don and doff during his ward rounds for the highrisk patients.
He is also waking at night with a fast, regular, “pounding” heartbeat and seemingly inexplicable episodes of “complete panic and agitation”.
In the last two weeks, he has needed to wake his wife on two occasions, so she could comfort him when he was uncontrollably agitated. He is completely perplexed as to how this could happen to him.
Your patient is a well-known, gentle specialist physician. He is renowned for his care of patients and their families. He is well known in the hospital for his support of nursing and ancillary staff, as well as the time taken on his rounds to teach the junior doctors in his team.
Since the onset of the COVID-19 pandemic, he has been busier than usual, both at the hospital and at his private rooms, where he spends one-quarter of his time. In March 2020, he and his colleagues, all in their 50s, calculated they were at approximately 2–3 per cent risk of death should they catch severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), the causative pathogen of coronavirus disease 2019 (COVID-19).
He had worked through the dark days of the pandemic, including 28 February 2020 when New Zealand confirmed its first case of COVID-19. He had experienced the lack of full PPE and the uncertainty of COVID-19 as it spread through patients during the level 4 lockdown from 26 March 2020. As with all healthcare workers, he had stoically carried on at work despite being frightened he might “bring the virus home” to his family.
While wanting to be a supporter of the national COVID-19 strategy, he is increasingly critical of the Government and Ministry of Health response, which he feels has been slow and poorly delivered. The Pfizer–BioNTech COVID-19 vaccination programme was rolled out in the UK from December 2020, whereas the first shipment of the vaccine – some 60,000 doses – did not arrive in New Zealand until 15 February.
He had waited in line until after the DHB board chairman received his first vaccination. Your patient then received his first dose in March and the second in April. However, he is very aware that a booster dose is needed six months after the second dose, and he is now experiencing the same stresses he felt in 2020, as it is now more than seven months since his second dose.
He is usually fit and well, and he is happily married with three healthy children. His past history is only of mild hypertension, which is treated with candesartan 16mg daily. He has never smoked and previously drank alcohol in a modest way, although admits to heavier drinking over the last few months.
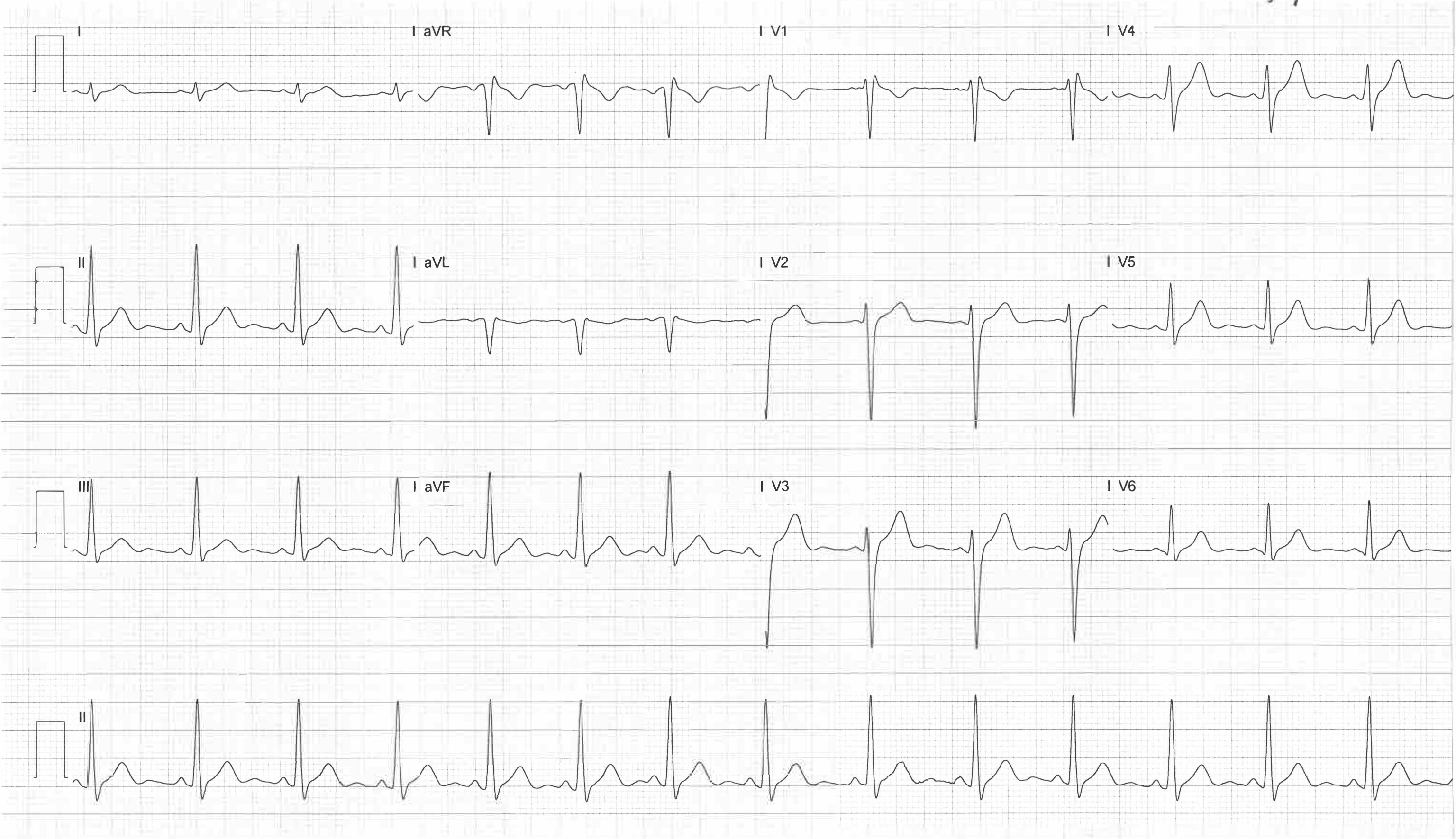
On examination, he is a pleasant, middle-aged man, although a little agitated as he discusses his problems. His blood pressure is 140/90mmHg, and he has a regular pulse at 90 beats per minute, with normal heart sounds. His chest is clear. A resting electrocardiogram is taken.
- What does the ECG show?
- What is the likely diagnosis?
- What would be your initial management plan?
- What is the evidence of waning effectiveness after the second dose of the Pfizer–BioNTech COVID-19 vaccine?
- What is the evidence of effectiveness of a booster dose of the Pfizer–BioNTech vaccine?
- How do you help your patient from here?






![Barbara Fountain, editor of New Zealand Doctor Rata Aotearoa, and Paul Hutchison, GP and senior medical clinician at Tāmaki Health [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/Barbara%20Fountain%2C%20editor%20of%20New%20Zealand%20Doctor%20Rata%20Aotearoa%2C%20and%20Paul%20Hutchison%2C%20GP%20and%20senior%20medical%20clinician%20at%20T%C4%81maki%20Health%20CR%20Simon%20Maude.jpg?itok=-HbQ1EYA)
![Lori Peters, NP and advanced health improvement practitioner at Mahitahi Hauora, and Jasper Nacilla, NP at The Terrace Medical Centre in Wellington [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/2.%20Lori%20Peters%2C%20NP%20and%20advanced%20HIP%20at%20Mahitahi%20Hauora%2C%20and%20Jasper%20Nacilla%2C%20NP%20at%20The%20Terrace%20Medical%20Centre%20in%20Wellington%20CR%20Simon%20Maude.jpg?itok=sUfbsSF1)
![Ministry of Social Development health and disability coordinator Liz Williams, regional health advisors Mary Mojel and Larah Takarangi, and health and disability coordinators Rebecca Staunton and Myint Than Htut [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/3.%20Ministry%20of%20Social%20Development%27s%20Liz%20Williams%2C%20Mary%20Mojel%2C%20Larah%20Takarangi%2C%20Rebecca%20Staunton%20and%20Myint%20Than%20Htut%20CR%20Simon%20Maude.jpg?itok=9ceOujzC)
![Locum GP Helen Fisher, with Te Kuiti Medical Centre NP Bridget Woodney [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/4.%20Locum%20GP%20Helen%20Fisher%2C%20with%20Te%20Kuiti%20Medical%20Centre%20NP%20Bridget%20Woodney%20CR%20Simon%20Maude.jpg?itok=TJeODetm)
![Ruby Faulkner, GPEP2, with David Small, GPEP3 from The Doctors Greenmeadows in Napier [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/5.%20Ruby%20Faulkner%2C%20GPEP2%2C%20with%20David%20Small%2C%20GPEP3%20from%20The%20Doctors%20Greenmeadows%20in%20Napier%20CR%20Simon%20Maude.jpg?itok=B0u4wsIs)
![Rochelle Langton and Libby Thomas, marketing advisors at the Medical Protection Society [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/6.%20Rochelle%20Langton%20and%20Libby%20Thomas%2C%20marketing%20advisors%20at%20the%20Medical%20Protection%20Society%20CR%20Simon%20Maude.jpg?itok=r52_Cf74)
![Specialist GP Lucy Gibberd, medical advisor at MPS, and Zara Bolam, urgent-care specialist at The Nest Health Centre in Inglewood [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/7.%20Specialist%20GP%20Lucy%20Gibberd%2C%20medical%20advisor%20at%20MPS%2C%20and%20Zara%20Bolam%2C%20urgent-care%20specialist%20at%20The%20Nest%20Health%20Centre%20in%20Inglewood%20CR%20Simon%20Maude.jpg?itok=z8eVoBU3)
![Olivia Blackmore and Trudee Sharp, NPs at Gore Health Centre, and Gaylene Hastie, NP at Queenstown Medical Centre [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/8.%20Olivia%20Blackmore%20and%20Trudee%20Sharp%2C%20NPs%20at%20Gore%20Health%20Centre%2C%20and%20Gaylene%20Hastie%2C%20NP%20at%20Queenstown%20Medical%20Centre%20CR%20Simon%20Maude.jpg?itok=Z6u9d0XH)
![Mary Toloa, specialist GP at Porirua and Union Community Health Service in Wellington, Mara Coler, clinical pharmacist at Tū Ora Compass Health, and Bhavna Mistry, specialist GP at Porirua and Union Community Health Service [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/9.%20Mary%20Toloa%2C%20Porirua%20and%20Union%20Community%20Health%20Service%20in%20Wellington%2C%20Mara%20Coler%2C%20T%C5%AB%20Ora%20Compass%20Health%2C%20and%20Bhavna%20Mistry%2C%20PUCHS%20CR%20Simon%20Maude.jpg?itok=kpChr0cc)