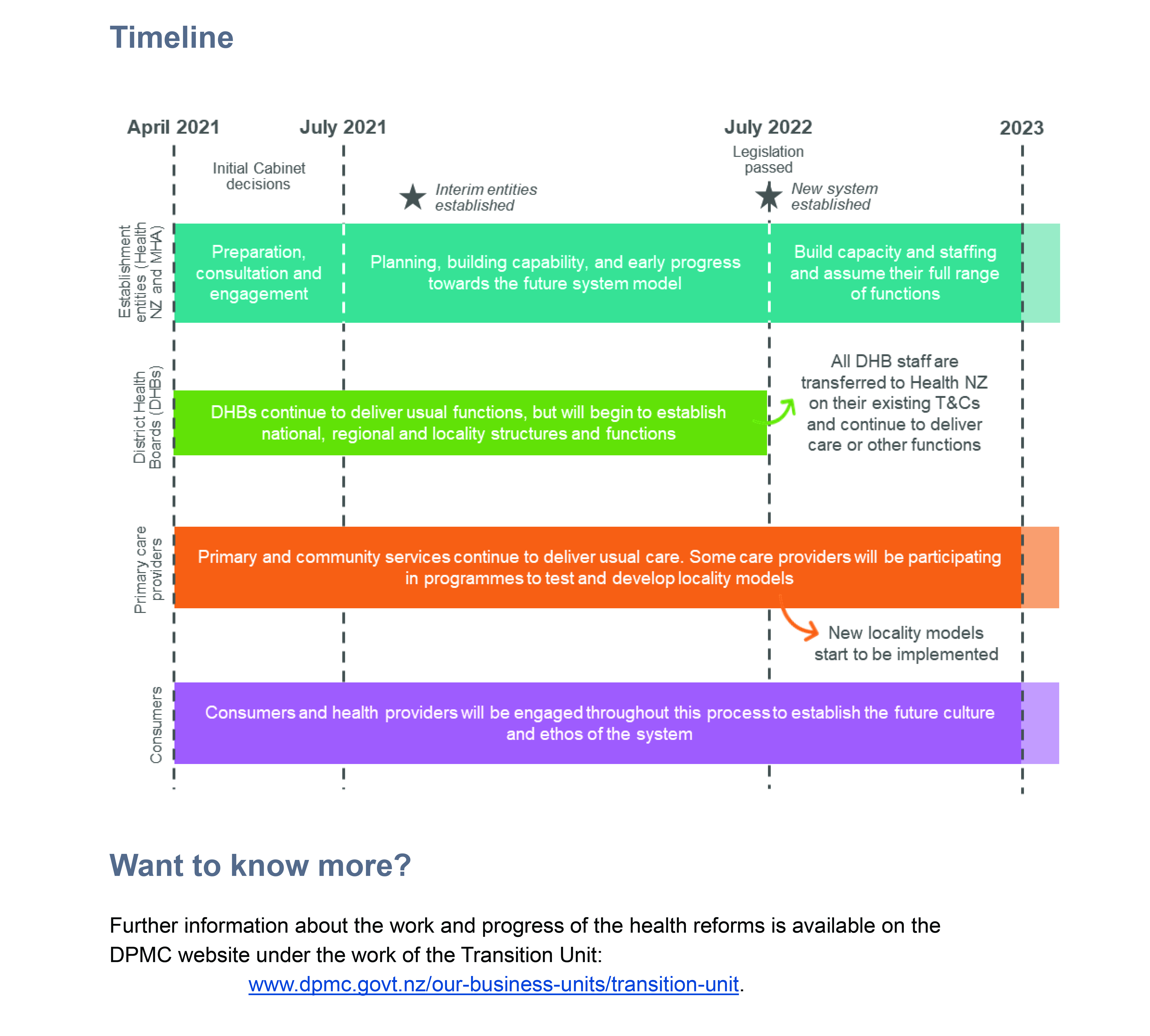
Primary and community services will be organised in locality networks, but the number of these has not been stated.
Mr Little said: “We are going to put the emphasis squarely on primary and community healthcare and will do away with duplication and unnecessary bureaucracy between regions, so that our health workers can do what they do best – keep people well.
“The reforms will mean that for the first time, we will have a truly national health system, and the kind of treatment people get will no longer be determined by where they live.”
New Zealand Doctor Rata Aotearoa asked Stephen McKernan, head of the Health and Disability System Transition Unit in the Department of the Prime Minister and Cabinet, who would own localities.
Mr McKernan said this would be determined by the commissioning function of Health NZ, in consultation with localities.
PHOs could support locality networks, Mr McKernan says, but would have to be a bit broader.
A locality would encompass aged residential care, pharmacy, home-based support services and other Tier 1 services as identified in the final report of the Health and Disability System Review Panel.
In the panel’s report, these were: GPs, pharmacists, midwives, allied health professionals, Māori and Pacific providers, dentists and dental therapists, home care workers, district nurses, community mental health services, public health nurses and aged-care providers.
The reforms were sparked by the review, but have gone further than its recommendations. For example, the review report said to slash the number of DHBs, not abolish them, and advocated a Māori Health Authority that had monitoring and advisory functions only.
How services are delivered will be based on locality plans, created with communities alongside Iwi-Māori Partnership Boards.
A health reform white paper, Our health and disability system, has additional notes on primary and community care.