How many birthing parents in Aotearoa New Zealand will now qualify for ACC funded care for maternal birth injuries?
Out of the approximately 60,000 people giving birth each year in New Zealand, about 30 per cent will have a caesarean section delivery (18,000). That leaves 70 per cent giving birth via spontaneous or instrumental vaginal delivery (42,000). Considering that up to 85 per cent of people who give birth vaginally sustain perineal trauma, it is estimated that up to 35,700 people per year will qualify for ACC funding for perineal tears alone.
These figures exclude the other birthing injuries also covered by ACC. Some of these injuries occur concurrently; some occur independently of each other.
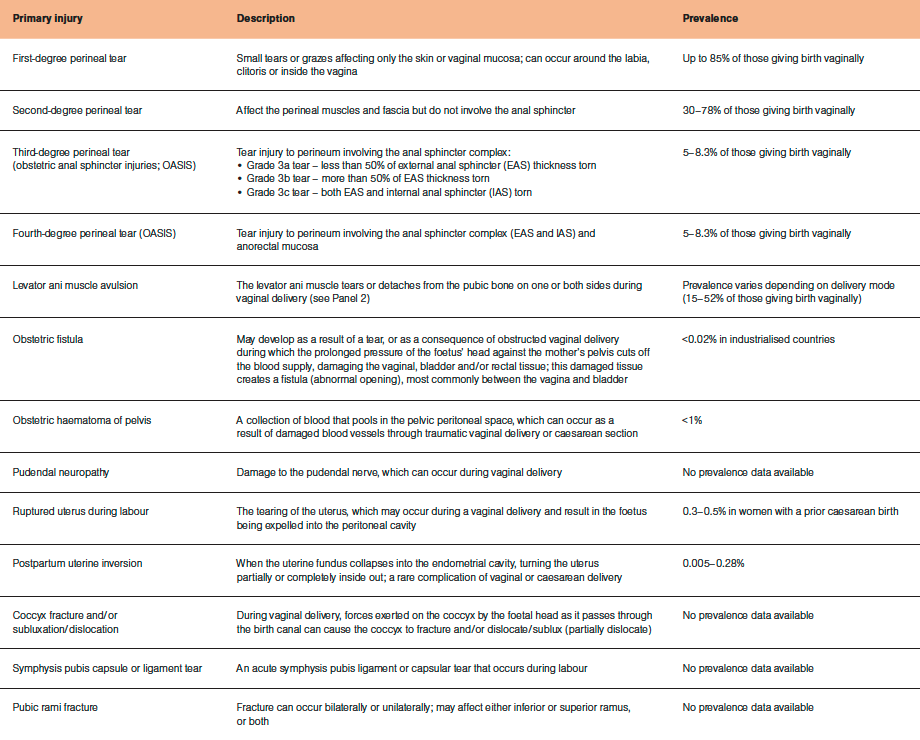
The table provides a summary of the primary maternal birth injuries and their prevalence. Consequential injuries are also summarised.
A proportion of these injuries will be diagnosed and treated immediately in the hospital setting, such as uterine inversion, ruptured uterus, obstetric haematoma and obstetric fistula.
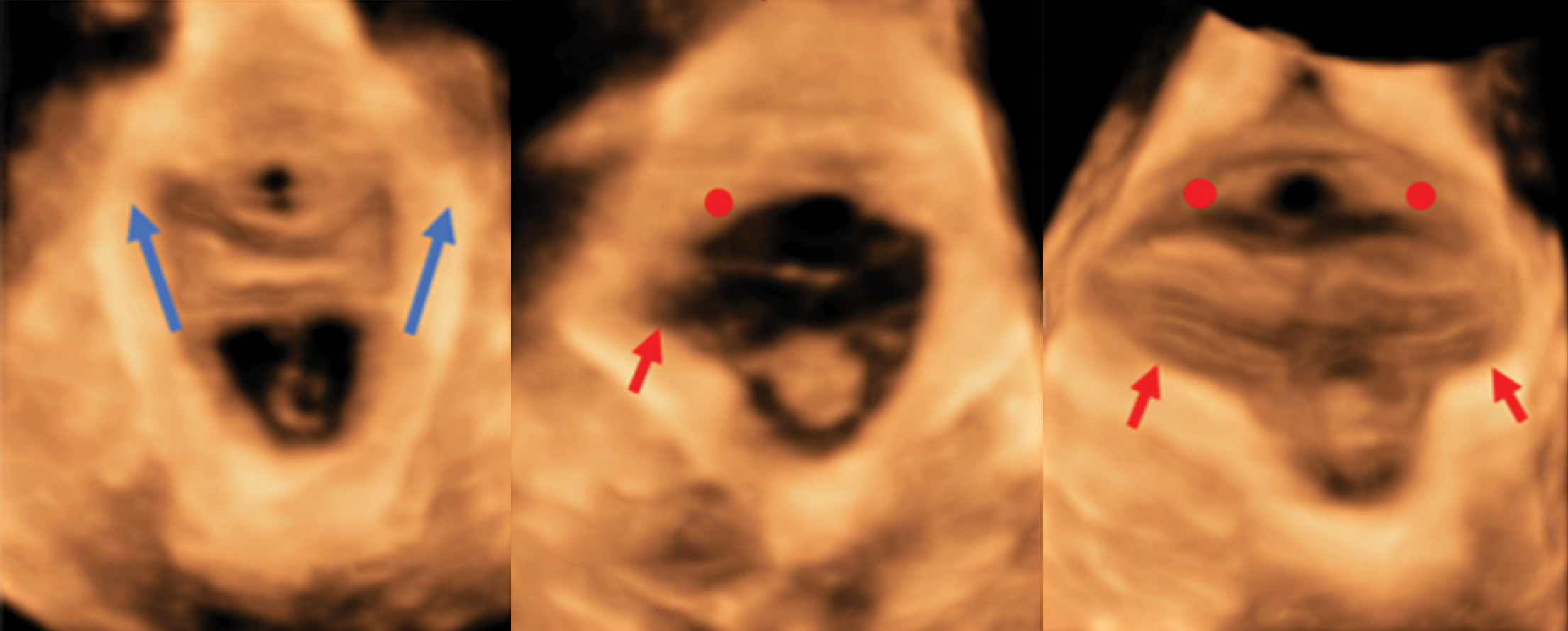
Other injuries will be noted to have occurred but may or may not be registered with ACC at the time of birth due to several factors. Injuries in this category include tears to the perineum, pudendal neuropathy, symphysis pubis dysfunctions, coccyx dysfunctions and pubic ramus fracture. Diagnosis of levator ani muscle avulsions take six to 12 months to confirm as there may be healing of partial avulsions (Panel 2 – see below).
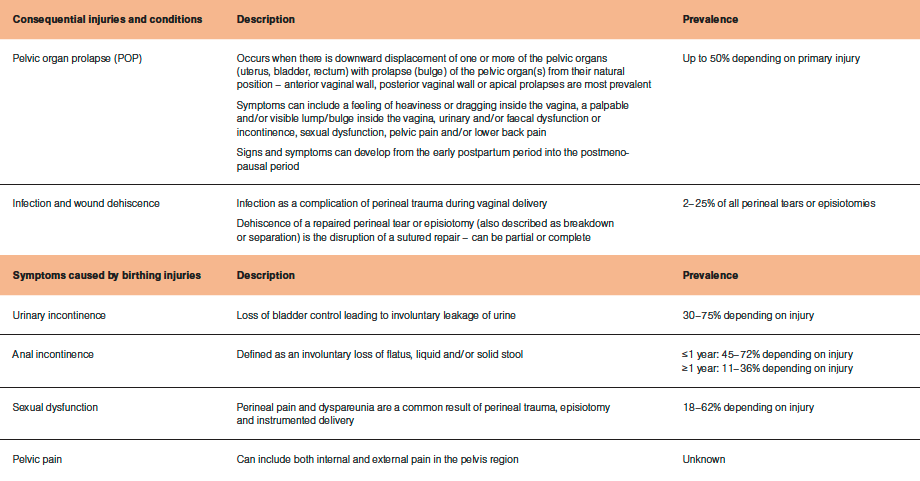
There are also consequential injuries of the primary injury (listed above) to consider, such as pelvic organ prolapse, infection and wound dehiscence. Symptoms of primary birthing injuries can include urinary and anal incontinence, pelvic pain and sexual dysfunction. While these symptoms alone are not considered to be injuries, they are caused by the primary injury and therefore receive coverage.
Depending on the birthing injury, ACC registration of most injuries can be completed by an obstetrician, gynaecologist, colorectal surgeon, GP, nurse practitioner, registered nurse or pelvic health physiotherapist. Midwives can only register perineal tears. Coccyx and symphysis pubis injuries can be registered by musculoskeletal physiotherapists, osteopaths or chiropractors.
See the ‘Maternal birth injuries’ page on the ACC website (acc.co.nz/for-providers/maternal-birth-injuries) for an easy summary sheet of who can register which injury.
As many injuries are not able to be registered by midwives, and birthing parents often do not develop symptoms of injury for weeks or months after birth, GPs and pelvic health physiotherapists need to be prepared to register the injuries.









![Barbara Fountain, editor of New Zealand Doctor Rata Aotearoa, and Paul Hutchison, GP and senior medical clinician at Tāmaki Health [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/Barbara%20Fountain%2C%20editor%20of%20New%20Zealand%20Doctor%20Rata%20Aotearoa%2C%20and%20Paul%20Hutchison%2C%20GP%20and%20senior%20medical%20clinician%20at%20T%C4%81maki%20Health%20CR%20Simon%20Maude.jpg?itok=-HbQ1EYA)
![Lori Peters, NP and advanced health improvement practitioner at Mahitahi Hauora, and Jasper Nacilla, NP at The Terrace Medical Centre in Wellington [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/2.%20Lori%20Peters%2C%20NP%20and%20advanced%20HIP%20at%20Mahitahi%20Hauora%2C%20and%20Jasper%20Nacilla%2C%20NP%20at%20The%20Terrace%20Medical%20Centre%20in%20Wellington%20CR%20Simon%20Maude.jpg?itok=sUfbsSF1)
![Ministry of Social Development health and disability coordinator Liz Williams, regional health advisors Mary Mojel and Larah Takarangi, and health and disability coordinators Rebecca Staunton and Myint Than Htut [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/3.%20Ministry%20of%20Social%20Development%27s%20Liz%20Williams%2C%20Mary%20Mojel%2C%20Larah%20Takarangi%2C%20Rebecca%20Staunton%20and%20Myint%20Than%20Htut%20CR%20Simon%20Maude.jpg?itok=9ceOujzC)
![Locum GP Helen Fisher, with Te Kuiti Medical Centre NP Bridget Woodney [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/4.%20Locum%20GP%20Helen%20Fisher%2C%20with%20Te%20Kuiti%20Medical%20Centre%20NP%20Bridget%20Woodney%20CR%20Simon%20Maude.jpg?itok=TJeODetm)
![Ruby Faulkner, GPEP2, with David Small, GPEP3 from The Doctors Greenmeadows in Napier [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/5.%20Ruby%20Faulkner%2C%20GPEP2%2C%20with%20David%20Small%2C%20GPEP3%20from%20The%20Doctors%20Greenmeadows%20in%20Napier%20CR%20Simon%20Maude.jpg?itok=B0u4wsIs)
![Rochelle Langton and Libby Thomas, marketing advisors at the Medical Protection Society [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/6.%20Rochelle%20Langton%20and%20Libby%20Thomas%2C%20marketing%20advisors%20at%20the%20Medical%20Protection%20Society%20CR%20Simon%20Maude.jpg?itok=r52_Cf74)
![Specialist GP Lucy Gibberd, medical advisor at MPS, and Zara Bolam, urgent-care specialist at The Nest Health Centre in Inglewood [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/7.%20Specialist%20GP%20Lucy%20Gibberd%2C%20medical%20advisor%20at%20MPS%2C%20and%20Zara%20Bolam%2C%20urgent-care%20specialist%20at%20The%20Nest%20Health%20Centre%20in%20Inglewood%20CR%20Simon%20Maude.jpg?itok=z8eVoBU3)
![Olivia Blackmore and Trudee Sharp, NPs at Gore Health Centre, and Gaylene Hastie, NP at Queenstown Medical Centre [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/8.%20Olivia%20Blackmore%20and%20Trudee%20Sharp%2C%20NPs%20at%20Gore%20Health%20Centre%2C%20and%20Gaylene%20Hastie%2C%20NP%20at%20Queenstown%20Medical%20Centre%20CR%20Simon%20Maude.jpg?itok=Z6u9d0XH)
![Mary Toloa, specialist GP at Porirua and Union Community Health Service in Wellington, Mara Coler, clinical pharmacist at Tū Ora Compass Health, and Bhavna Mistry, specialist GP at Porirua and Union Community Health Service [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/9.%20Mary%20Toloa%2C%20Porirua%20and%20Union%20Community%20Health%20Service%20in%20Wellington%2C%20Mara%20Coler%2C%20T%C5%AB%20Ora%20Compass%20Health%2C%20and%20Bhavna%20Mistry%2C%20PUCHS%20CR%20Simon%20Maude.jpg?itok=kpChr0cc)