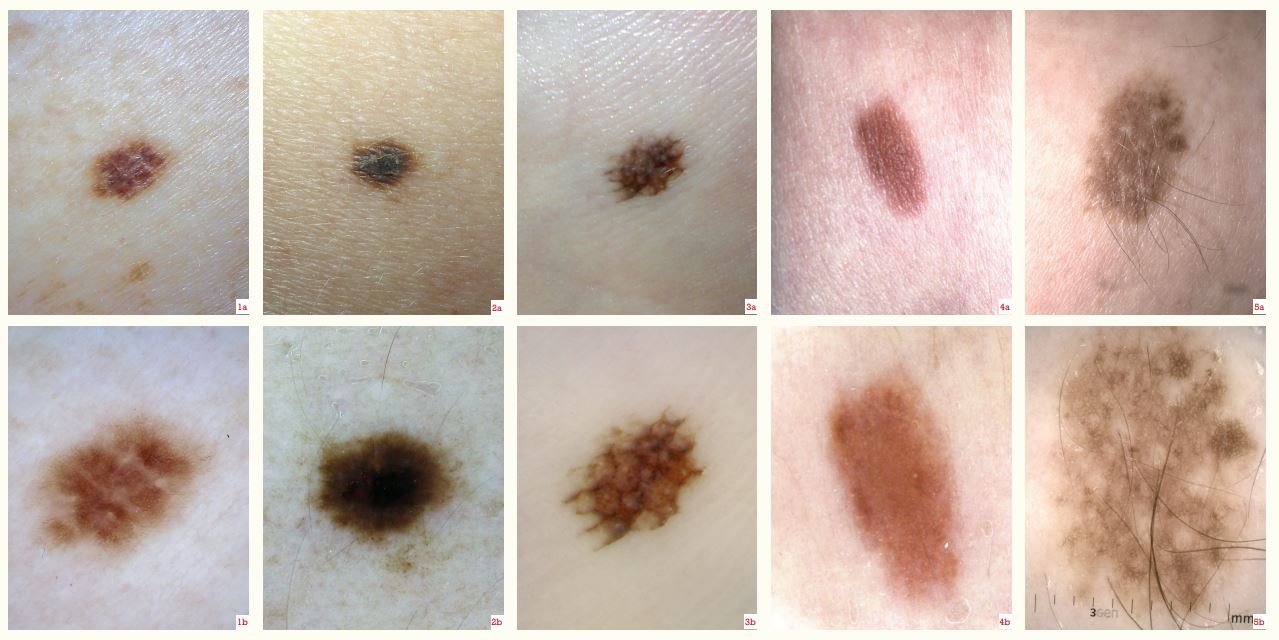
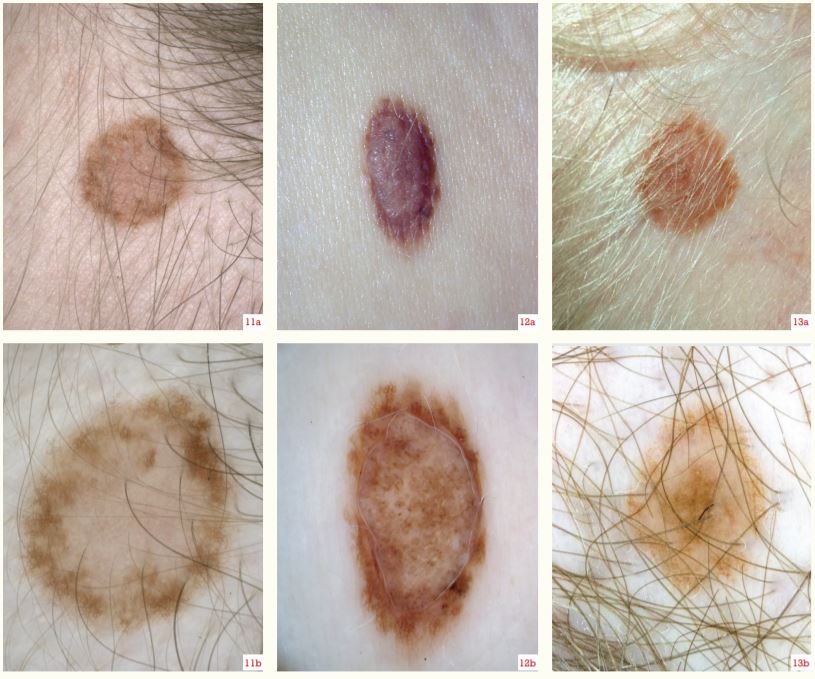
Examination of a naevus with a dermatoscope allows an evaluation of the global pattern and focal features.
Junctional naevi – are recognised by a reticular pattern of lines in most areas (Figures 1b and 2b) and by parallel lines on the palms and soles (Figure 3b), or they appear structureless. The lines fade peripherally.
Dermal naevi – are structureless (Figures 4b, 8b, 9b and 10b) or are made up of clods, which are small and separated (Figure 6b), or large (Figure 7b). Keratin plugs may be seen as orange/brown, irregularly distributed, superficial clods (Figure 7b). Facial, non-pigmented dermal naevi have faint to prominent, curved or serpiginous, non-branched vessels (Figures 8b and 9b).
Compound naevi – have both features, symmetrically distributed as two patterns (Figures 11b and 12b) or three concentric patterns (Figure 13b). The dermal component may not be clearly seen (Figure 5b; in this example, perifollicular hypopigmentation and thick hair growth indicate the naevus is of congenital pattern and will have a dermal component).
Naevi have particular dermatoscopic characteristics according to site, especially noticeable on the scalp (Figures 11b and 13b; an annular pattern is common), face (Figures 8b, 9b and 10b), and palm/sole (Figure 3b; a parallel furrow pattern, best appreciated on the lesion edge).