Therefore, not unjust and unfair. And, therefore, not inequitable. Gross
The report was developed to inform the development of a New Zealand Health Plan 2024–2027 (which will be published later) but has “many other uses and benefits”. As the report notes, it is non-traditional because it doesn’t include service user or community perspectives – but both will be included next time. In particular, “information on broader Māori perspectives of health and wellbeing and holistic concepts that are deeply important to Māori is limited”.
It is clear from the report’s introduction that it has other limitations, too. These are mostly related to having to use the data available, even if not perfect (as is the case of ethnicity, with evidence that Māori are systematically undercounted in NHI ethnicity data).3 There are also limitations where data essentially doesn’t exist (as is the case with data about the health of tāngata whaikaha/ disabled people).
In the early pages of the report, the emphasis appears to be on describing inequities in health outcomes between population groups. In doing so, the report repeats the Ministry of Health definition of equity: “In Aotearoa New Zealand, people have differences in health that are not only avoidable but unfair and unjust. Equity recognises different people with different levels of advantage require different approaches and resources to get equitable health outcomes.”4
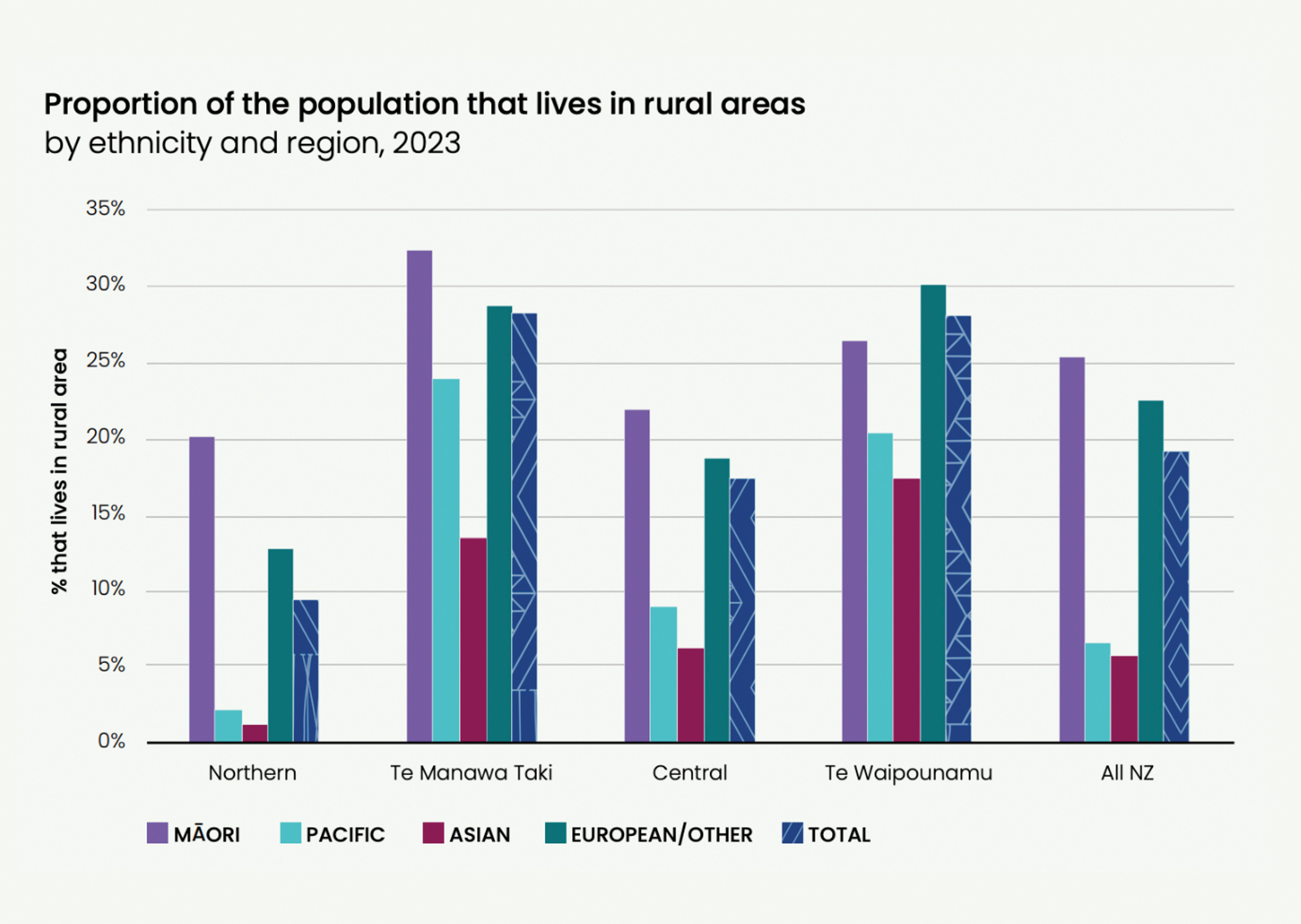
As you go through the report, you can see helpful, clearly presented, information on all sorts of topics. I was especially taken with the data on rurality. We are often told that rural populations have inequities compared with more urban populations, and sometimes, this feels like it is a tactic to say ethnic inequities aren’t that bad because inequities affect other people, too. But the data emphasises an intersection between rurality and ethnicity – with Māori making up the highest proportion of the rural population of any ethnic group in three of the four regions of Aotearoa. Without data, we can only imagine the additional impacts of rurality for Māori with lived experience of disability.
But when I got to the life expectancy section, I was stopped in my tracks. It is not news that the differences in life expectancy between Māori and non-Māori/non-Pacific populations are unfair and unjust, but it continues to be awful. The report quantifies this as Māori women dying, on average, seven years earlier than European/Other women and Māori men eight years earlier than European/ Other men.
The report digs into this further by providing an overview of the factors contributing to the life expectancy gap between Māori and Pacific people compared with non-Māori/non-Pacific people.
These factors are split into four groups: amenable only, preventable only, amenable and preventable, and (gasp) non-avoidable. Between one and three years of the life expectancy gap for Māori is classed as non-avoidable (depending on what part of Aotearoa you live).
The terms amenable and preventable are discussed in the body of the report. Avoidable mortality is deaths occurring in those aged 0–74 years (excluding stillbirths) that could potentially have been avoided. Prevention includes successful public health promotion such as Smokefree legislation, alcohol harm reduction and injury prevention. But non-avoidable? What is that? The only description is in the section on ICD-10 codes5 where non-avoidable is “all other deaths not listed in the above in all age groups”.








![Barbara Fountain, editor of New Zealand Doctor Rata Aotearoa, and Paul Hutchison, GP and senior medical clinician at Tāmaki Health [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/Barbara%20Fountain%2C%20editor%20of%20New%20Zealand%20Doctor%20Rata%20Aotearoa%2C%20and%20Paul%20Hutchison%2C%20GP%20and%20senior%20medical%20clinician%20at%20T%C4%81maki%20Health%20CR%20Simon%20Maude.jpg?itok=-HbQ1EYA)
![Lori Peters, NP and advanced health improvement practitioner at Mahitahi Hauora, and Jasper Nacilla, NP at The Terrace Medical Centre in Wellington [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/2.%20Lori%20Peters%2C%20NP%20and%20advanced%20HIP%20at%20Mahitahi%20Hauora%2C%20and%20Jasper%20Nacilla%2C%20NP%20at%20The%20Terrace%20Medical%20Centre%20in%20Wellington%20CR%20Simon%20Maude.jpg?itok=sUfbsSF1)
![Ministry of Social Development health and disability coordinator Liz Williams, regional health advisors Mary Mojel and Larah Takarangi, and health and disability coordinators Rebecca Staunton and Myint Than Htut [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/3.%20Ministry%20of%20Social%20Development%27s%20Liz%20Williams%2C%20Mary%20Mojel%2C%20Larah%20Takarangi%2C%20Rebecca%20Staunton%20and%20Myint%20Than%20Htut%20CR%20Simon%20Maude.jpg?itok=9ceOujzC)
![Locum GP Helen Fisher, with Te Kuiti Medical Centre NP Bridget Woodney [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/4.%20Locum%20GP%20Helen%20Fisher%2C%20with%20Te%20Kuiti%20Medical%20Centre%20NP%20Bridget%20Woodney%20CR%20Simon%20Maude.jpg?itok=TJeODetm)
![Ruby Faulkner, GPEP2, with David Small, GPEP3 from The Doctors Greenmeadows in Napier [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/5.%20Ruby%20Faulkner%2C%20GPEP2%2C%20with%20David%20Small%2C%20GPEP3%20from%20The%20Doctors%20Greenmeadows%20in%20Napier%20CR%20Simon%20Maude.jpg?itok=B0u4wsIs)
![Rochelle Langton and Libby Thomas, marketing advisors at the Medical Protection Society [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/6.%20Rochelle%20Langton%20and%20Libby%20Thomas%2C%20marketing%20advisors%20at%20the%20Medical%20Protection%20Society%20CR%20Simon%20Maude.jpg?itok=r52_Cf74)
![Specialist GP Lucy Gibberd, medical advisor at MPS, and Zara Bolam, urgent-care specialist at The Nest Health Centre in Inglewood [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/7.%20Specialist%20GP%20Lucy%20Gibberd%2C%20medical%20advisor%20at%20MPS%2C%20and%20Zara%20Bolam%2C%20urgent-care%20specialist%20at%20The%20Nest%20Health%20Centre%20in%20Inglewood%20CR%20Simon%20Maude.jpg?itok=z8eVoBU3)
![Olivia Blackmore and Trudee Sharp, NPs at Gore Health Centre, and Gaylene Hastie, NP at Queenstown Medical Centre [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/8.%20Olivia%20Blackmore%20and%20Trudee%20Sharp%2C%20NPs%20at%20Gore%20Health%20Centre%2C%20and%20Gaylene%20Hastie%2C%20NP%20at%20Queenstown%20Medical%20Centre%20CR%20Simon%20Maude.jpg?itok=Z6u9d0XH)
![Mary Toloa, specialist GP at Porirua and Union Community Health Service in Wellington, Mara Coler, clinical pharmacist at Tū Ora Compass Health, and Bhavna Mistry, specialist GP at Porirua and Union Community Health Service [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/9.%20Mary%20Toloa%2C%20Porirua%20and%20Union%20Community%20Health%20Service%20in%20Wellington%2C%20Mara%20Coler%2C%20T%C5%AB%20Ora%20Compass%20Health%2C%20and%20Bhavna%20Mistry%2C%20PUCHS%20CR%20Simon%20Maude.jpg?itok=kpChr0cc)