For Māori, appearing in more than one group compounds the disadvantage
There is a well-established link between oral health and systemic health. Therefore, optimising oral healthcare should be a concern of all those involved in healthcare delivery. Sometimes, dental problems may not be obvious to health professionals, especially in older people.1
The case for access to funded dental services in New Zealand has been promoted for many years.2 It is another area where health inequity pervades for Māori.3 The impact of inaccessibility can extend across groups with disability, lower socioeconomic status, mental health conditions and geographic isolation. For Māori, appearing in more than one group compounds the disadvantage.
Until a national solution is delivered, it is important that health professionals who aren’t dental specialists regularly consider the place of oral care in overall health delivery.
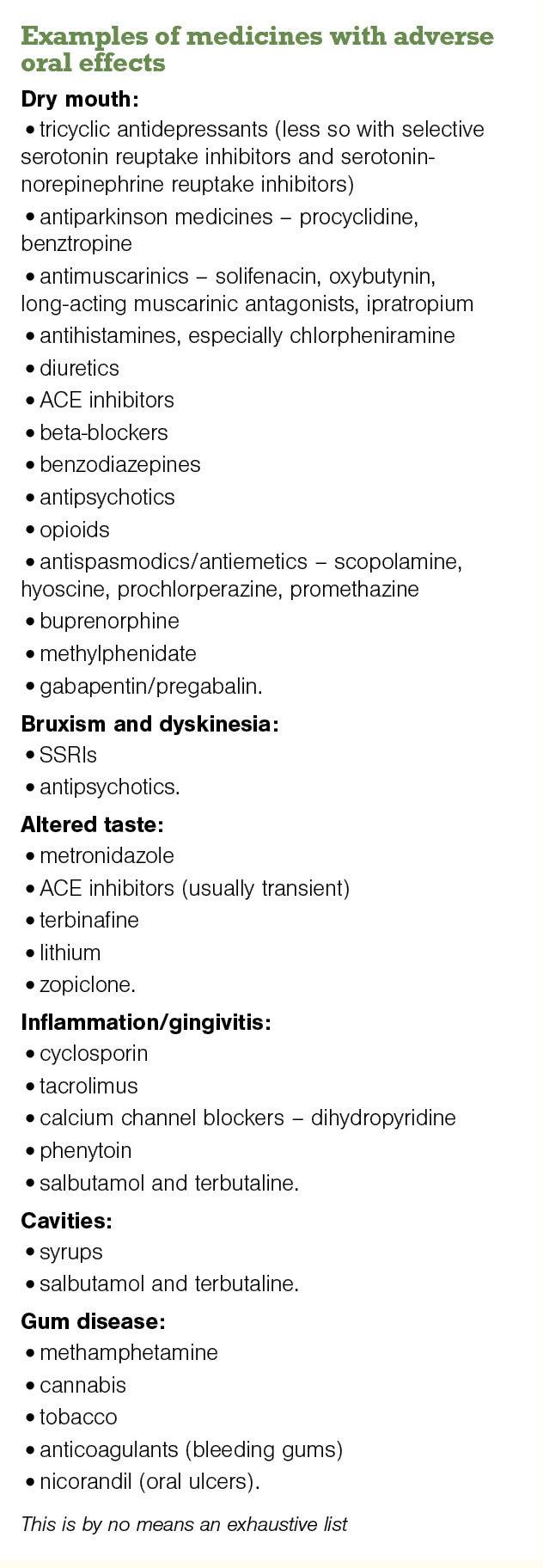
Medicines can affect oral health in a variety of ways (see panel). Hyposalivation is one identified mechanism, with saliva having antimicrobial activity that helps to prevent tooth decay and tooth wear. Saliva is also essential to digestion, swallowing and speech.
Many drugs are reported to cause salivary gland hypofunction, leading to xerostomia. Muscarinic acetylcholine receptors (M1, M3) and alpha-1 and beta-1 adrenergic receptors on saliva secretory cells mediate salivary secretion. Medicines that inhibit these receptors can decrease saliva flow.
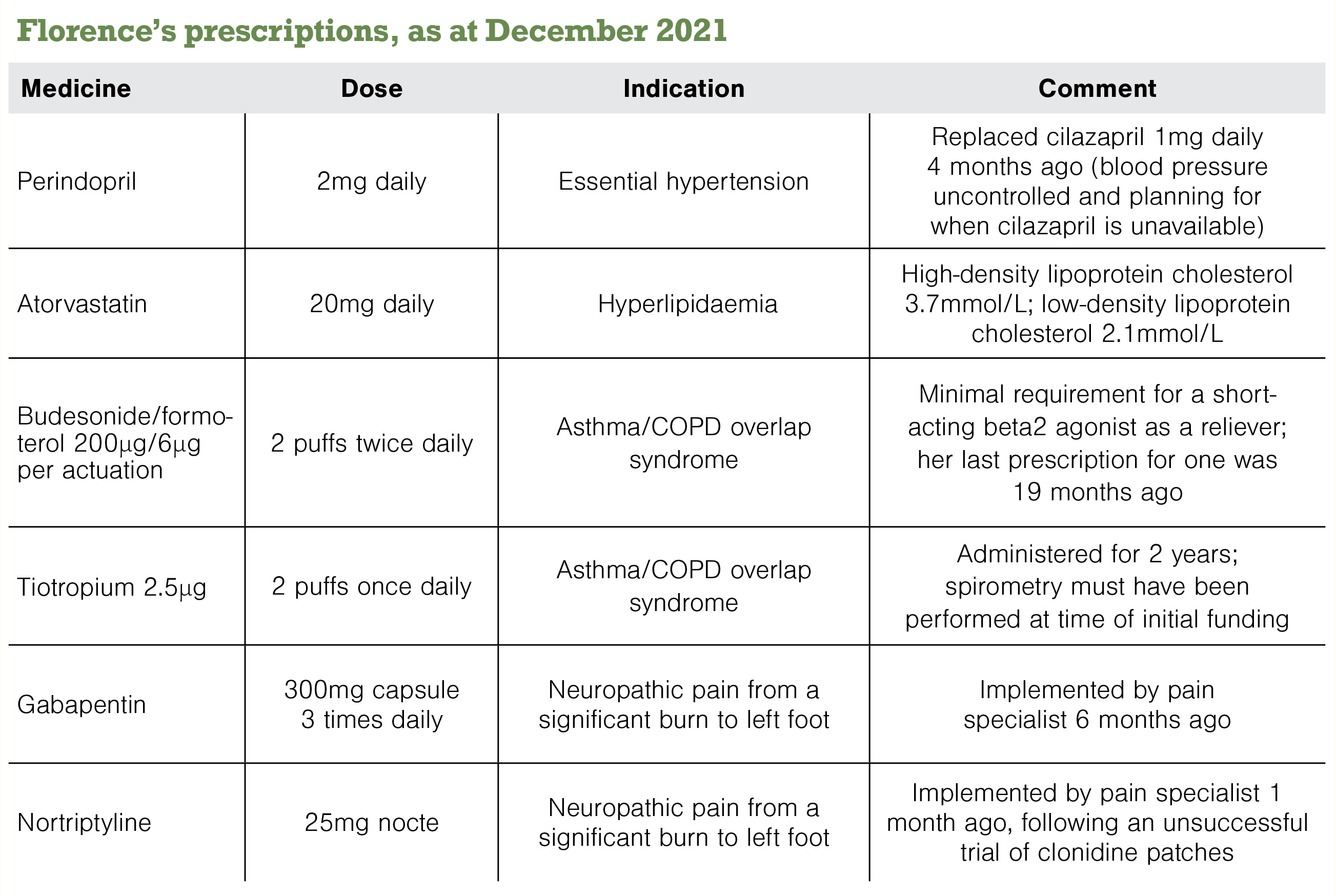
Florence confirms her mouth has felt dry for some months and may have gotten worse over the last month. Her approach to deal with this has been to suck on boiled, sugary sweets. Her children have commented that she seems to never be without a lolly.
Considering the anticholinergic burden of medicines is a reasonable place to start.
The ACB Calculator (acbcalc.com) can help indicate the risk of anticholinergic impact when making prescribing decisions – nortriptyline is given an anticholinergic burden rating that is “high risk”. This risk extends to more than oral health.
Other medicines with an ACB high-risk rating include antipsychotics (eg, clozapine and olanzapine) and medicines for urinary frequency and incontinence (eg, oxybutynin and solifenacin).
The list of medicines causing salivary gland hypofunction and xerostomia is, however, significantly wider than those inhibiting parasympathetic activity (tinyurl.com/MedsSaliva).4
Clonidine (a centrally acting anti-adrenergic agent) and gabapentin (for which a high level of evidence also exists to cause xerostomia) were implicated when Florence first noticed symptoms. Considering alternate medicines to those with high risk should be factored in if possible.
The other medicines in Florence’s regimen to bear in mind are tiotropium5 (a long-acting muscarinic antagonist) and perindopril. ACE inhibitors can directly cause dry mouth and lichenoid sensitivity reactions.6
A further consideration for Florence with respect to oral healthcare is the budesonide, which can cause pharyngitis, oral mucositis and candidiasis, particularly in older people.






![Barbara Fountain, editor of New Zealand Doctor Rata Aotearoa, and Paul Hutchison, GP and senior medical clinician at Tāmaki Health [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/Barbara%20Fountain%2C%20editor%20of%20New%20Zealand%20Doctor%20Rata%20Aotearoa%2C%20and%20Paul%20Hutchison%2C%20GP%20and%20senior%20medical%20clinician%20at%20T%C4%81maki%20Health%20CR%20Simon%20Maude.jpg?itok=-HbQ1EYA)
![Lori Peters, NP and advanced health improvement practitioner at Mahitahi Hauora, and Jasper Nacilla, NP at The Terrace Medical Centre in Wellington [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/2.%20Lori%20Peters%2C%20NP%20and%20advanced%20HIP%20at%20Mahitahi%20Hauora%2C%20and%20Jasper%20Nacilla%2C%20NP%20at%20The%20Terrace%20Medical%20Centre%20in%20Wellington%20CR%20Simon%20Maude.jpg?itok=sUfbsSF1)
![Ministry of Social Development health and disability coordinator Liz Williams, regional health advisors Mary Mojel and Larah Takarangi, and health and disability coordinators Rebecca Staunton and Myint Than Htut [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/3.%20Ministry%20of%20Social%20Development%27s%20Liz%20Williams%2C%20Mary%20Mojel%2C%20Larah%20Takarangi%2C%20Rebecca%20Staunton%20and%20Myint%20Than%20Htut%20CR%20Simon%20Maude.jpg?itok=9ceOujzC)
![Locum GP Helen Fisher, with Te Kuiti Medical Centre NP Bridget Woodney [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/4.%20Locum%20GP%20Helen%20Fisher%2C%20with%20Te%20Kuiti%20Medical%20Centre%20NP%20Bridget%20Woodney%20CR%20Simon%20Maude.jpg?itok=TJeODetm)
![Ruby Faulkner, GPEP2, with David Small, GPEP3 from The Doctors Greenmeadows in Napier [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/5.%20Ruby%20Faulkner%2C%20GPEP2%2C%20with%20David%20Small%2C%20GPEP3%20from%20The%20Doctors%20Greenmeadows%20in%20Napier%20CR%20Simon%20Maude.jpg?itok=B0u4wsIs)
![Rochelle Langton and Libby Thomas, marketing advisors at the Medical Protection Society [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/6.%20Rochelle%20Langton%20and%20Libby%20Thomas%2C%20marketing%20advisors%20at%20the%20Medical%20Protection%20Society%20CR%20Simon%20Maude.jpg?itok=r52_Cf74)
![Specialist GP Lucy Gibberd, medical advisor at MPS, and Zara Bolam, urgent-care specialist at The Nest Health Centre in Inglewood [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/7.%20Specialist%20GP%20Lucy%20Gibberd%2C%20medical%20advisor%20at%20MPS%2C%20and%20Zara%20Bolam%2C%20urgent-care%20specialist%20at%20The%20Nest%20Health%20Centre%20in%20Inglewood%20CR%20Simon%20Maude.jpg?itok=z8eVoBU3)
![Olivia Blackmore and Trudee Sharp, NPs at Gore Health Centre, and Gaylene Hastie, NP at Queenstown Medical Centre [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/8.%20Olivia%20Blackmore%20and%20Trudee%20Sharp%2C%20NPs%20at%20Gore%20Health%20Centre%2C%20and%20Gaylene%20Hastie%2C%20NP%20at%20Queenstown%20Medical%20Centre%20CR%20Simon%20Maude.jpg?itok=Z6u9d0XH)
![Mary Toloa, specialist GP at Porirua and Union Community Health Service in Wellington, Mara Coler, clinical pharmacist at Tū Ora Compass Health, and Bhavna Mistry, specialist GP at Porirua and Union Community Health Service [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/9.%20Mary%20Toloa%2C%20Porirua%20and%20Union%20Community%20Health%20Service%20in%20Wellington%2C%20Mara%20Coler%2C%20T%C5%AB%20Ora%20Compass%20Health%2C%20and%20Bhavna%20Mistry%2C%20PUCHS%20CR%20Simon%20Maude.jpg?itok=kpChr0cc)