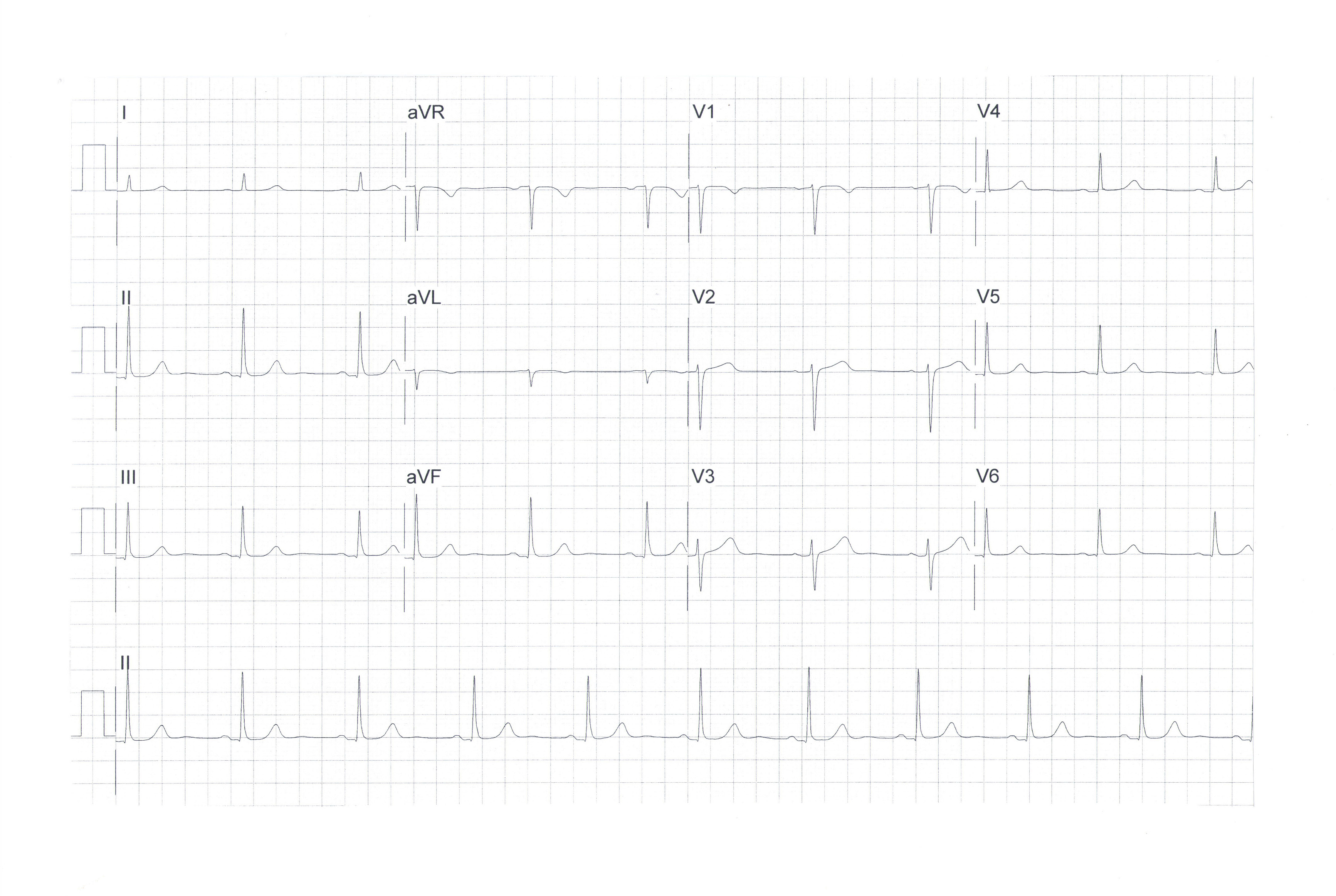
1. The ECG shows sinus rhythm, a rate of 63 beats per minute and a normal axis. It is normal, as are most ECGs when patients present with upper abdominal/lower chest pains, particularly if the pains are not ongoing when the ECG is performed.
2. No! Patients who present with upper abdominal/lower chest pain are common, and their symptoms are notoriously difficult for clinicians to accurately diagnose.
a. If the chest pain is provoked with exercise, it is more likely to be ischaemic. At rest, or when a patient is lying down, it is more likely to be from reflux or gastritis, or to have a musculoskeletal cause, or one of very many alternative causes.
If there is radiation of pain to the arms or throat, this might suggest an ischaemic origin, but other causes of pain can also radiate, so certainty is not obtained from this feature either. If the pain lasts less than 10 to 15 minutes, this might suggest ischaemia, but many other causes of chest pain are also transient and repetitive.
If the pain is relieved by a glyceryl trinitrate spray, this might assist the diagnosis of cardiac ischaemia, but oesophageal spasm, among other sources of upper abdominal/lower chest pain, can also be relieved by a GTN spray.
3. A screen of blood tests can be of considerable help with the diagnosis. A full blood count can help exclude a gastric bleed or point towards an infection, such as pneumonia or shingles, or pyelonephritis if the white blood cells are raised. Creatinine and electrolyte levels may focus the diagnosis to a renal or ureteric problem, or, if the sodium level is low, to possible heart failure.
A serum lipase or amylase test may assist with the diagnosis of pancreatitis or gall stone biliary colic. A creatine kinase level may assist with diagnosis of muscular problems or myocardial damage within the last few days.
Liver function tests may help diagnose biliary colic or cholecystitis, an acute hepatitis or hepatic abscess. A D-dimer test may help raise the likelihood of a pulmonary embolus, and a high cholesterol level may make a vascular event (coronary or aortic) more likely.
A high serum glucose or HBA1c level may point towards an infection, ischaemia or even pancreatitis. An N-terminal pro B-type natriuretic peptide test may help focus on the heart for heart failure, or a pericarditis or myocarditis. An elevated C-reactive protein level may suggest inflammation in one of very many organs, or a generalised inflammatory condition such as systemic lupus erythematosus.
A troponin test may help detect cardiac damage, which can result from ischaemia or myocyte damage from another cause, such as a chronic tropinaemia related to renal failure. If the troponin level is raised, it would suggest a lower threshold for hospital admission, which would usually be the safe option for the patient. There are many other blood tests that could also potentially help.
4. Imaging tests are many and could be of help. A plain chest or abdominal x-ray, back x-rays, a chest and abdominal CT scan, a CT pulmonary angiogram, a transthoracic or transoesophageal echocardiogram, an upper abdominal ultrasound scan, a cardiac, chest and abdominal MRI scan, a gastroscopy and colonoscopy, and a pill camera assessment of the small bowel are some that come to immediate mind, but the list is extensive…and largely unobtainable for a clinician trying to make a bedside diagnosis for a patient.
5. In theory, the patient could be admitted to hospital for a further opinion, ECG monitoring, blood tests, a chest x-ray and further tests that seem relevant to the hospital team (see above). However, in practice, this is not possible.
You are aware that the hospital service is severely short of beds, nurses and doctors. Admitting your patient is simply not realistic unless you are very seriously concerned about the possibility of an acute coronary syndrome or severe, acute ill health. You recognise that it is you who has to make the decision about the likely diagnosis and the list of possible alternative diagnoses.
You also understand that it is you who will need to worry about the clinical decision you make, and that, on occasion, you will get this wrong. You are trained to do this and prepared to stand up to your responsibilities, despite the very difficult healthcare environment in which you work.
6. Clinicians are currently over-worked, often exhausted, with high levels of burnout, which does reduce their ability to optimally assess and manage difficult medical presentations. GPs who are the backbone of the health service as currently structured, as well as hospital clinicians who maintain 24/7 cover of their speciality areas and also run busy outpatient clinics, work very hard to optimally assess their patients. They work in a healthcare system that is underresourced in every clinical area.
Where the ministry could give clinicians considerable assistance is to ensure that the important work of the HDC is responsive to the very, very major deficiencies within the service, and not unduly critical when errors occur, which they surely must do in the current structure. Defensive and worse practice of medicine will result from unrealistic expectations of clinicians who work in this very difficult health structure.
7. Of course! Clinicians are human and vulnerable. Every clinician will make some diagnostic errors despite very careful practice. It is the nature of medicine, but certainly exacerbated by the serious issues mentioned above.
a. It is important to have an HDC able to convince bedside clinicians that it truly understands the limitations to optimal practice of medicine within the current healthcare climate – that it understands the very difficult decisions being made by highly skilled clinicians and is aware of the environment in which medicine in New Zealand is actually practiced.
This would relieve some of the stresses felt by clinicians trying to care for the next patient, the next patient, and the next patient with an upper abdominal/lower chest pain presentation, and not wishing to then be criticised by the HDC process.






![Barbara Fountain, editor of New Zealand Doctor Rata Aotearoa, and Paul Hutchison, GP and senior medical clinician at Tāmaki Health [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/Barbara%20Fountain%2C%20editor%20of%20New%20Zealand%20Doctor%20Rata%20Aotearoa%2C%20and%20Paul%20Hutchison%2C%20GP%20and%20senior%20medical%20clinician%20at%20T%C4%81maki%20Health%20CR%20Simon%20Maude.jpg?itok=-HbQ1EYA)
![Lori Peters, NP and advanced health improvement practitioner at Mahitahi Hauora, and Jasper Nacilla, NP at The Terrace Medical Centre in Wellington [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/2.%20Lori%20Peters%2C%20NP%20and%20advanced%20HIP%20at%20Mahitahi%20Hauora%2C%20and%20Jasper%20Nacilla%2C%20NP%20at%20The%20Terrace%20Medical%20Centre%20in%20Wellington%20CR%20Simon%20Maude.jpg?itok=sUfbsSF1)
![Ministry of Social Development health and disability coordinator Liz Williams, regional health advisors Mary Mojel and Larah Takarangi, and health and disability coordinators Rebecca Staunton and Myint Than Htut [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/3.%20Ministry%20of%20Social%20Development%27s%20Liz%20Williams%2C%20Mary%20Mojel%2C%20Larah%20Takarangi%2C%20Rebecca%20Staunton%20and%20Myint%20Than%20Htut%20CR%20Simon%20Maude.jpg?itok=9ceOujzC)
![Locum GP Helen Fisher, with Te Kuiti Medical Centre NP Bridget Woodney [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/4.%20Locum%20GP%20Helen%20Fisher%2C%20with%20Te%20Kuiti%20Medical%20Centre%20NP%20Bridget%20Woodney%20CR%20Simon%20Maude.jpg?itok=TJeODetm)
![Ruby Faulkner, GPEP2, with David Small, GPEP3 from The Doctors Greenmeadows in Napier [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/5.%20Ruby%20Faulkner%2C%20GPEP2%2C%20with%20David%20Small%2C%20GPEP3%20from%20The%20Doctors%20Greenmeadows%20in%20Napier%20CR%20Simon%20Maude.jpg?itok=B0u4wsIs)
![Rochelle Langton and Libby Thomas, marketing advisors at the Medical Protection Society [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/6.%20Rochelle%20Langton%20and%20Libby%20Thomas%2C%20marketing%20advisors%20at%20the%20Medical%20Protection%20Society%20CR%20Simon%20Maude.jpg?itok=r52_Cf74)
![Specialist GP Lucy Gibberd, medical advisor at MPS, and Zara Bolam, urgent-care specialist at The Nest Health Centre in Inglewood [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/7.%20Specialist%20GP%20Lucy%20Gibberd%2C%20medical%20advisor%20at%20MPS%2C%20and%20Zara%20Bolam%2C%20urgent-care%20specialist%20at%20The%20Nest%20Health%20Centre%20in%20Inglewood%20CR%20Simon%20Maude.jpg?itok=z8eVoBU3)
![Olivia Blackmore and Trudee Sharp, NPs at Gore Health Centre, and Gaylene Hastie, NP at Queenstown Medical Centre [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/8.%20Olivia%20Blackmore%20and%20Trudee%20Sharp%2C%20NPs%20at%20Gore%20Health%20Centre%2C%20and%20Gaylene%20Hastie%2C%20NP%20at%20Queenstown%20Medical%20Centre%20CR%20Simon%20Maude.jpg?itok=Z6u9d0XH)
![Mary Toloa, specialist GP at Porirua and Union Community Health Service in Wellington, Mara Coler, clinical pharmacist at Tū Ora Compass Health, and Bhavna Mistry, specialist GP at Porirua and Union Community Health Service [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/9.%20Mary%20Toloa%2C%20Porirua%20and%20Union%20Community%20Health%20Service%20in%20Wellington%2C%20Mara%20Coler%2C%20T%C5%AB%20Ora%20Compass%20Health%2C%20and%20Bhavna%20Mistry%2C%20PUCHS%20CR%20Simon%20Maude.jpg?itok=kpChr0cc)