Since the initial cardiovascular risk tables were developed by Aotearoa New Zealand’s epidemiologist Rod Jackson, we have altered our thinking about treating cardiovascular risk.
Initially, statins were relatively expensive medicines, so use was restricted to secondary prevention and very-high-risk primary prevention. This was a cost-effectiveness decision to target those people at greatest risk, although statins are effective even at lower cardiovascular risk. The studies at the time looked at total cholesterol and LDL cholesterol levels, rather than total cardiovascular risk, and found that any LDL reduction was beneficial.
By 2018, the new Aotearoa New Zealand guidelines, Cardiovascular Disease Risk Assessment and Management for Primary Care, meant that not only did we have a country-specific calculator (PREDICT) but statins were considerably less expensive; hence, the lowering of the threshold for treatment.
The Ministry of Health’s 2018 guidelines recommend we should discuss the use of a statin with people who have a five-year cardiovascular risk of 5 to 15 per cent, particularly those in the higher end of that spectrum.1
While cardiovascular risk is an excellent tool to assist with treatment decisions because it encourages us to focus holistically and treat all risk factors, the treatment of dyslipidaemia itself is changing. There had always been discord between using the total cholesterol to HDL cholesterol ratio as a trigger for treatment and then using the LDL cholesterol level as the target for treatment.
The UK’s National Institute for Health and Care Excellence (NICE) guidance previously recommended that people with a 10-year risk of a cardiovascular event of more than 10 per cent (approximately 5 per cent five-year risk) be offered a statin. That threshold remains in the 2023 guidance, but it also recommends a more person-centred approach by considering a statin for people with a 10-year cardiovascular risk of “less than 10 per cent if they have an informed preference for taking a statin or there is concern that risk may be underestimated”.2
The guidance states that if more people took statins, there would be a greater reduction in CVD events – it is estimated that for every 1000 people with a 5 per cent 10-year risk who take a statin, the statin will prevent approximately 20 people from having a cardiovascular event in this time; and for those with a 10 per cent 10-year risk, the statin will prevent about 40 people from having a cardiovascular event.3
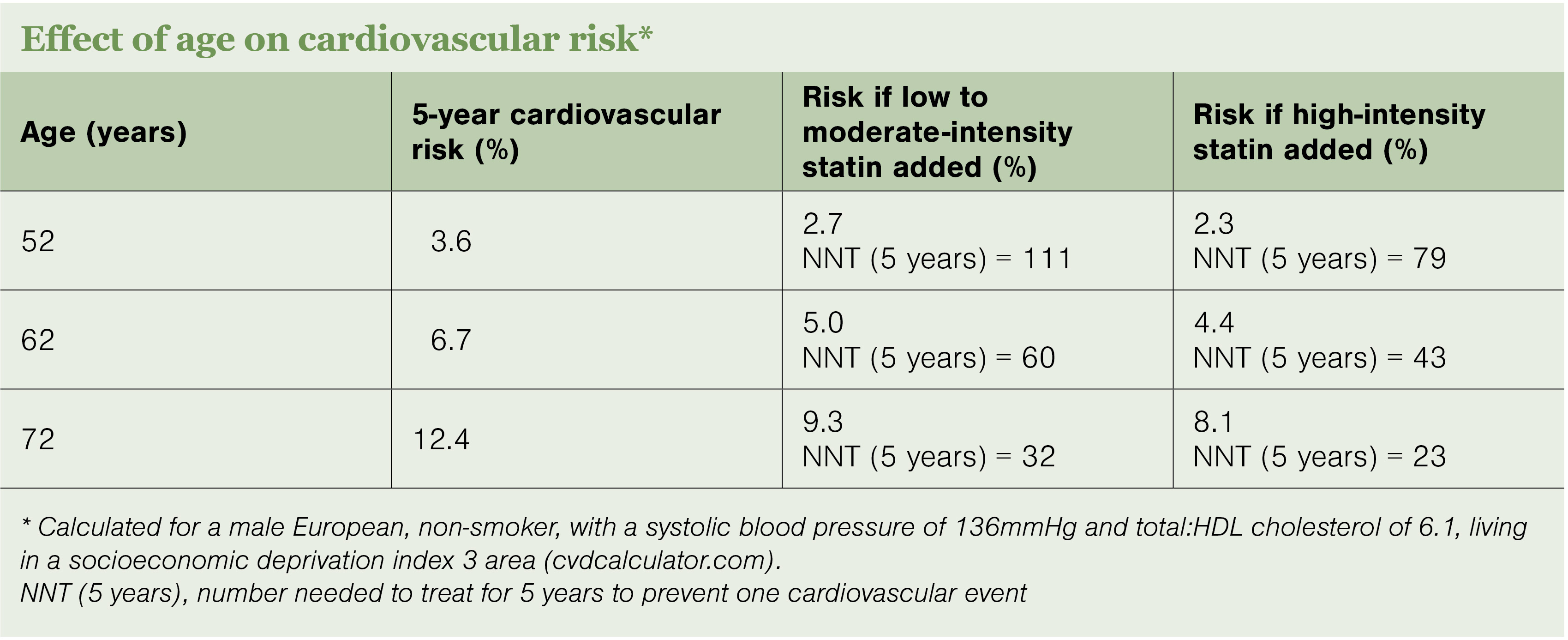
Applying this to the New Zealand environment is perhaps a matter of changing our perception of when to more actively advocate for the introduction of a statin. A hangover from the 1990s and early 2000s is the perception that we should wait until the five-year cardiovascular risk is closer to 10 per cent before starting a statin, but with the new evidence, having a more intense discussion when the five-year cardiovascular risk is around 5 per cent would be recommended. In particular, this is important for younger people and those with higher LDL cholesterol levels (eg, over 4.0mmol/L).
Importantly for Māori and Pacific peoples, the risk of CVD is higher than for Europeans, and CVD occurs at a younger age, so the implications of starting a statin early are even greater.