This is an area that lends itself to a set-piece conversation in your team. Everyone in the team – owners, managers, employees, clinicians and non-clinicians – can help plan and implement a set-piece response to various immunisation scenarios, just as a team might plan for and coordinate a scrum, corner kick or throw-in during a sports game.
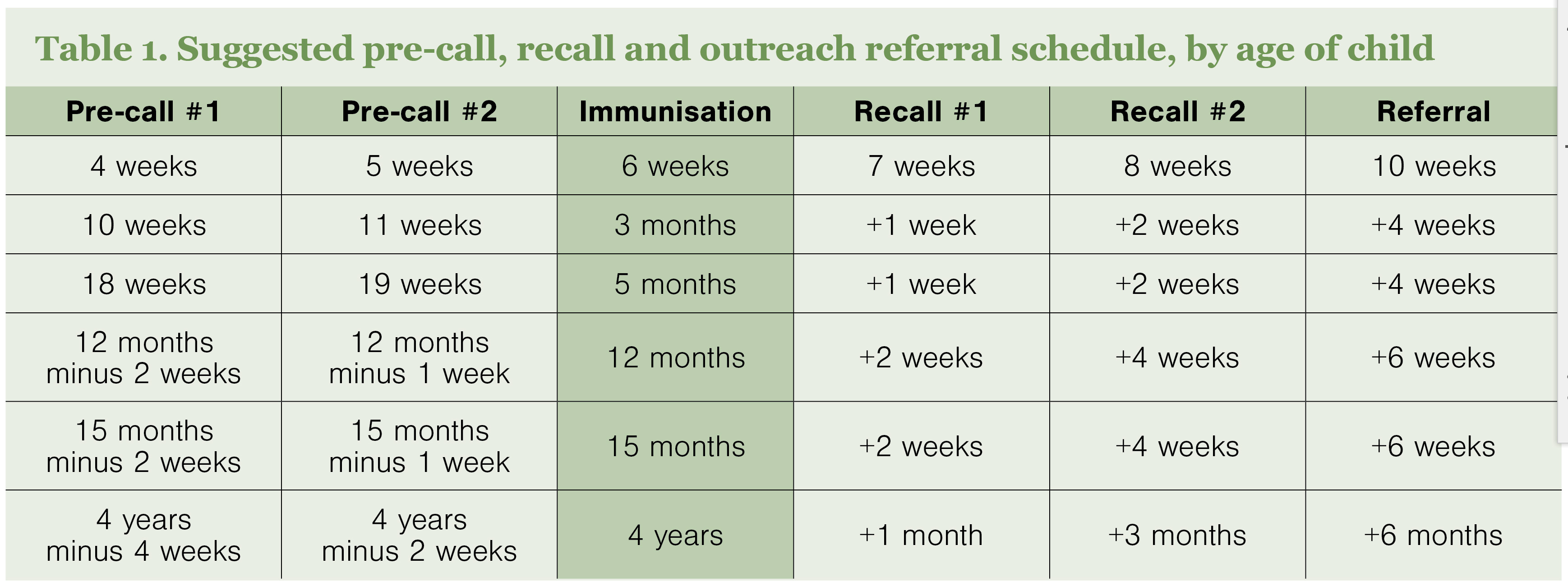
You know people are going to need pre-call and recall for immunisations, they are going to come in seeking immunisations, and people who need immunisations are going to come for other reasons.
Take an hour to sit down together and discuss what each person currently says and does with each step in the immunisation process. I can guarantee there will be variations in approach in any clinical team. Decide as a group if these variations are important, and if they lead to significant confusion among patients.
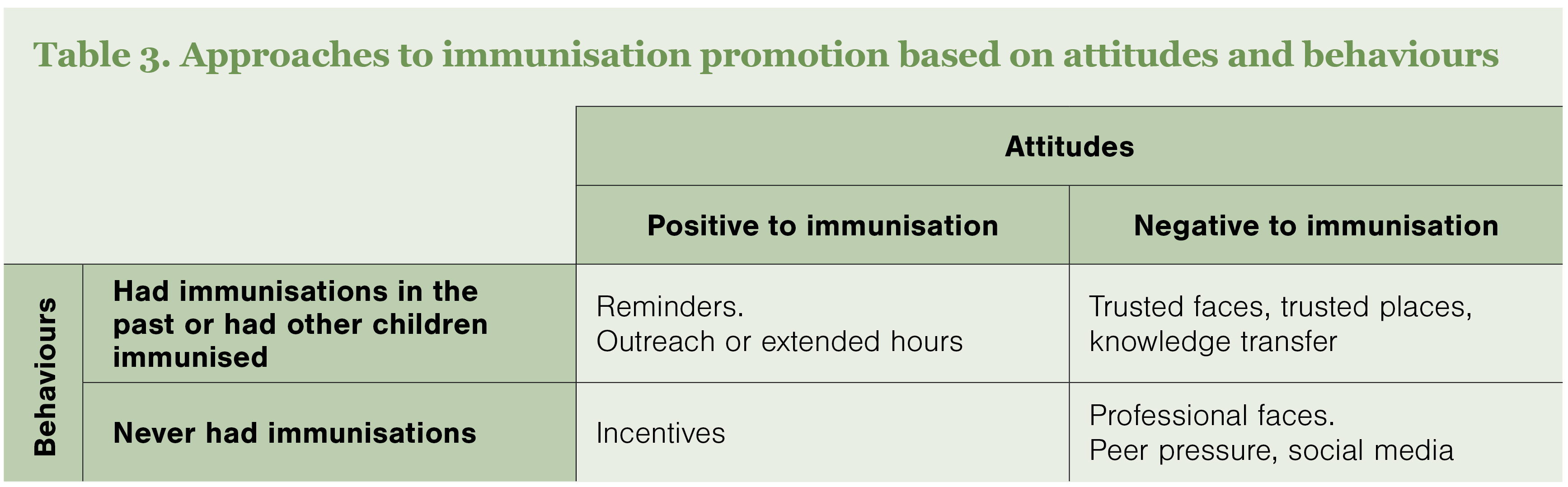
One clinician might never mention immunisation during a consultation because they don’t want to antagonise patients; another might make it a priority for every consultation. How does this impact patients in your practice when they see different clinicians on different days?
One nurse might send a text message, another an email, and another only ever call patients on the pre-call/recall list. How does this impact patient engagement?
Does your practice reach out when a notification of a new birth is received? A simple congratulations card can be a lovely gesture that makes a connection with a family and reminds them that you care and are there for them.