Losartan may offset the serum uric acid-increasing effects of other medicines
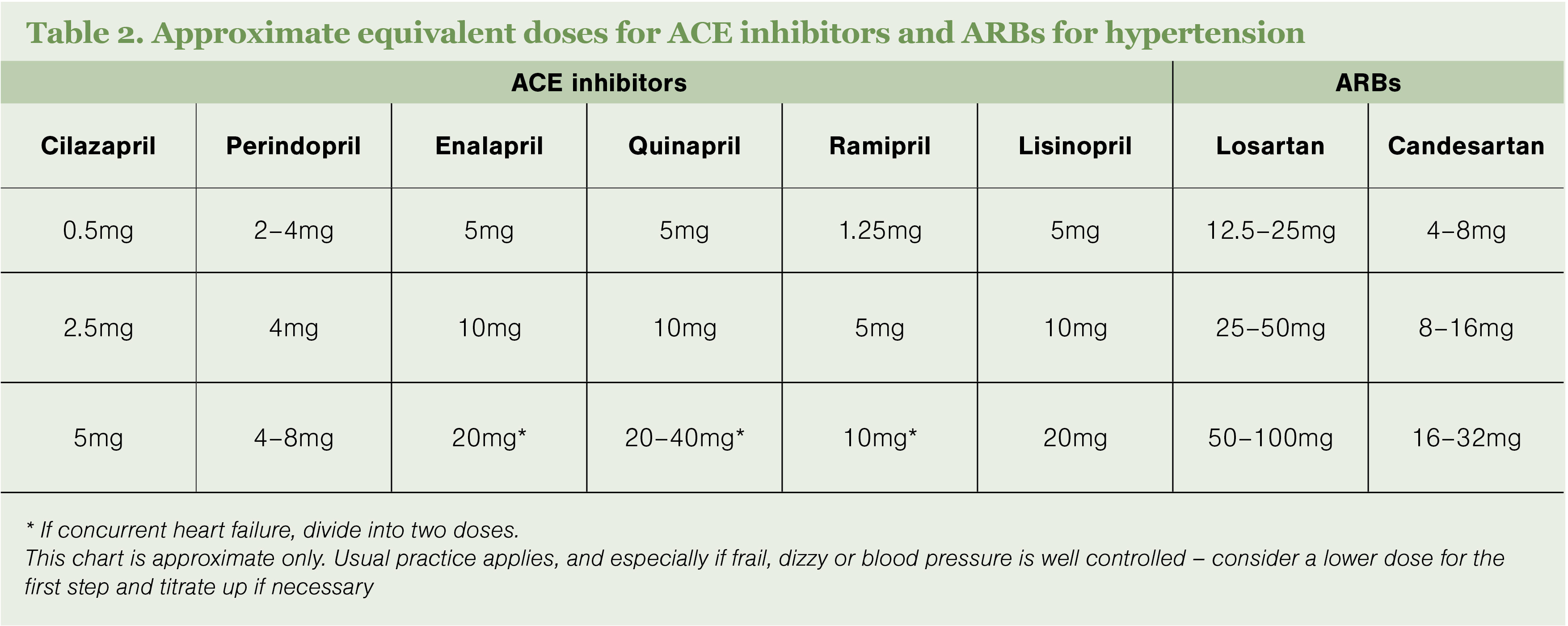
People taking cilazapril need to be switched to an alternative ACE inhibitor or an angiotensin receptor blocker (ARB) by mid-2023. At such time, cilazapril will become delisted due to the potential for supply issues. It may be important to reassure people that this change is not due to any concerns regarding cilazapril’s effectiveness or any newly discovered adverse effects.
There is no exact alternative to cilazapril. Most ACE inhibitors are similar and essentially interchangeable as their differences are small. Most ACE inhibitors and ARBs are similar in effectiveness, but there are some prescribing considerations and possible interpatient variability in tolerability. In addition, most ACE inhibitors can be taken once daily for hypertension, but some should be taken twice daily for heart failure, which may influence the choice of medicine. It can be helpful to ask the person what they would prefer and consider adherence.
Historically, ACE inhibitors had the greater evidence base over ARBs, with the latter prescribed if the person didn’t tolerate an ACE inhibitor. However, early studies did not allow a direct comparison between ACE inhibitors and ARBs. Subsequent meta-analyses showed no significant difference in the primary outcomes of acute myocardial infarction, heart failure, stroke or composite cardiovascular events between treatment groups, but fewer reports of adverse effects from ARBs.1,2
Many clinicians now prefer to start a person directly on an ARB to avoid potential side effects of ACE inhibitors, as these result in reluctance to take medicines and may lead to non-adherence and inequitable outcomes.
The most common adverse effect of ACE inhibitors is cough, which can occur in 5–20 per cent of people up to two years after initiation. If cough occurs, a change to an ARB is warranted. Cough associated with ARBs is approximately 65–75 per cent lower than with ACE inhibitors.
Angio-oedema is a rare but serious adverse effect of ACE inhibitors, with an incidence of 0.3 per cent (of which 20 per cent is severe), whereas the incidence with ARBs is much lower at approximately 0.1 per cent. Angio-oedema may also present atypically, with less acute, localised or mild symptoms, intermittent abdominal pain, or isolated limb swelling. This may occur years after initiation.
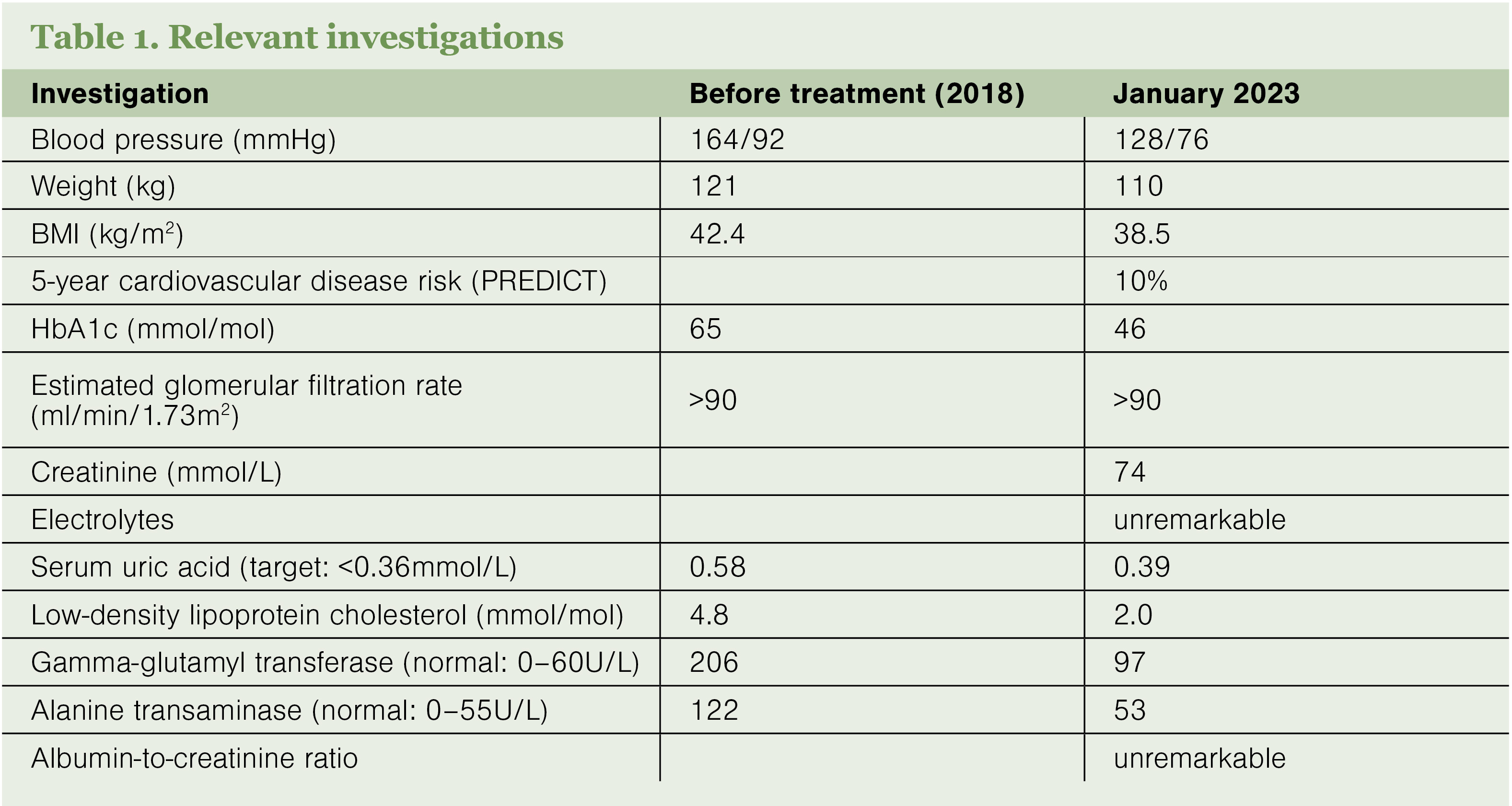
Losartan is an alternative to consider if the person has gout. Losartan is the only ARB (or ACE inhibitor) that has a demonstrated uricosuric effect. However, this is subject to pharmacogenomic variation, with resultant serum uric acid (SUA) lowering of up to 20 per cent. Even allowing for variation, losartan may offset the SUA-increasing effects of other medicines, such as thiazides, when used as an add on (but not replacement) for allopurinol or other gout preventers.
Although there is some variation between individual studies, the overall evidence for renal protection in people with hypertension and pre-existing albuminuria is not significantly different between ACE inhibitors and ARBs.3–6 However, diabetic nephropathy is currently only an approved use for losartan, not candesartan, in people with type 2 diabetes in Aotearoa New Zealand.
An additional consideration is that empagliflozin reduces the baseline risk of progression to end-stage kidney disease by approximately one-third. This is such a large effect compared with ACE inhibitors and ARBs that any difference between the classes would not be clinically relevant if empagliflozin is being taken.
In heart failure with reduced ejection fraction, the guidance is for an angiotensin receptor–neprilysin inhibitor as first-line therapy, with an ACE inhibitor or ARB if ARNIs are not tolerated.7 An important consideration when changing agents is that the treatment targets for ACE inhibitors and ARBs in heart failure differ from those in hypertension, as the dose is titrated to the maximum tolerated rather than to a blood pressure target. Further, close monitoring is required to avoid decompensation.
For people with concurrent heart failure with reduced ejection fraction, empagliflozin reduces the risk of cardiovascular death or hospitalisation for heart failure by 25 per cent, and that of any heart failure hospitalisations by 30 per cent.8 So, again, any differences between ACE inhibitors and ARBs would not be clinically significant if empagliflozin is being taken. However, these people may require closer monitoring during a medication change.






![Barbara Fountain, editor of New Zealand Doctor Rata Aotearoa, and Paul Hutchison, GP and senior medical clinician at Tāmaki Health [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/Barbara%20Fountain%2C%20editor%20of%20New%20Zealand%20Doctor%20Rata%20Aotearoa%2C%20and%20Paul%20Hutchison%2C%20GP%20and%20senior%20medical%20clinician%20at%20T%C4%81maki%20Health%20CR%20Simon%20Maude.jpg?itok=-HbQ1EYA)
![Lori Peters, NP and advanced health improvement practitioner at Mahitahi Hauora, and Jasper Nacilla, NP at The Terrace Medical Centre in Wellington [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/2.%20Lori%20Peters%2C%20NP%20and%20advanced%20HIP%20at%20Mahitahi%20Hauora%2C%20and%20Jasper%20Nacilla%2C%20NP%20at%20The%20Terrace%20Medical%20Centre%20in%20Wellington%20CR%20Simon%20Maude.jpg?itok=sUfbsSF1)
![Ministry of Social Development health and disability coordinator Liz Williams, regional health advisors Mary Mojel and Larah Takarangi, and health and disability coordinators Rebecca Staunton and Myint Than Htut [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/3.%20Ministry%20of%20Social%20Development%27s%20Liz%20Williams%2C%20Mary%20Mojel%2C%20Larah%20Takarangi%2C%20Rebecca%20Staunton%20and%20Myint%20Than%20Htut%20CR%20Simon%20Maude.jpg?itok=9ceOujzC)
![Locum GP Helen Fisher, with Te Kuiti Medical Centre NP Bridget Woodney [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/4.%20Locum%20GP%20Helen%20Fisher%2C%20with%20Te%20Kuiti%20Medical%20Centre%20NP%20Bridget%20Woodney%20CR%20Simon%20Maude.jpg?itok=TJeODetm)
![Ruby Faulkner, GPEP2, with David Small, GPEP3 from The Doctors Greenmeadows in Napier [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/5.%20Ruby%20Faulkner%2C%20GPEP2%2C%20with%20David%20Small%2C%20GPEP3%20from%20The%20Doctors%20Greenmeadows%20in%20Napier%20CR%20Simon%20Maude.jpg?itok=B0u4wsIs)
![Rochelle Langton and Libby Thomas, marketing advisors at the Medical Protection Society [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/6.%20Rochelle%20Langton%20and%20Libby%20Thomas%2C%20marketing%20advisors%20at%20the%20Medical%20Protection%20Society%20CR%20Simon%20Maude.jpg?itok=r52_Cf74)
![Specialist GP Lucy Gibberd, medical advisor at MPS, and Zara Bolam, urgent-care specialist at The Nest Health Centre in Inglewood [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/7.%20Specialist%20GP%20Lucy%20Gibberd%2C%20medical%20advisor%20at%20MPS%2C%20and%20Zara%20Bolam%2C%20urgent-care%20specialist%20at%20The%20Nest%20Health%20Centre%20in%20Inglewood%20CR%20Simon%20Maude.jpg?itok=z8eVoBU3)
![Olivia Blackmore and Trudee Sharp, NPs at Gore Health Centre, and Gaylene Hastie, NP at Queenstown Medical Centre [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/8.%20Olivia%20Blackmore%20and%20Trudee%20Sharp%2C%20NPs%20at%20Gore%20Health%20Centre%2C%20and%20Gaylene%20Hastie%2C%20NP%20at%20Queenstown%20Medical%20Centre%20CR%20Simon%20Maude.jpg?itok=Z6u9d0XH)
![Mary Toloa, specialist GP at Porirua and Union Community Health Service in Wellington, Mara Coler, clinical pharmacist at Tū Ora Compass Health, and Bhavna Mistry, specialist GP at Porirua and Union Community Health Service [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/9.%20Mary%20Toloa%2C%20Porirua%20and%20Union%20Community%20Health%20Service%20in%20Wellington%2C%20Mara%20Coler%2C%20T%C5%AB%20Ora%20Compass%20Health%2C%20and%20Bhavna%20Mistry%2C%20PUCHS%20CR%20Simon%20Maude.jpg?itok=kpChr0cc)