Informed consent
To give informed consent, Ricky needs to fully understand what GAHT entails, including the potential benefits, risks and irreversibility of GAHT. Patients report a wide range of responses and reactions from their support networks, and this understandably impacts on their wellbeing.
Mental health screening
As TNB patients are more likely to experience mental health issues, a mental health screening assessment is important. Treat any mental health issues in Ricky as you would for any other patient, and refer for more specialised support or assessment as needed. Ensure any mental health issue is well supported before starting GAHT, keeping in mind that this should never be a barrier to accessing hormones.
Wider psychosocial implications
Encourage Ricky to discuss the wider psychosocial implications of transition with a mental health practitioner. This does not need to be a psychiatrist or psychologist, but any mental health provider with expertise in the area. Although a “readiness assessment” was previously a prerequisite to accessing GAHT, health providers in Aotearoa, as in other countries, are moving towards an informed consent model where a formal assessment is no longer required.
Unless you feel this work is within your scope and expertise, refer Ricky to someone in your area who does this work regularly. This information should be visible on your local health pathway. In my experience, the majority of patients embarking on GAHT find these conversations really useful, and as a GP, I really appreciate the support another health provider can offer.
If this expert support is not funded in your area, consider utilising local funding pathways, such as “improved access” or even Work and Income funding if needed, or seeing if a national provider such as OUTLine (outline.org.nz) might be able to provide this support remotely. Ricky might also be keen to connect with other people who are taking GAHT through local or online support groups.
Binding
Check in to see if he is having any issues with binding. The long-term use of binders, particularly if they are too tight, can lead to pain in the spine and chest area, breathing issues, and even rib fractures and permanent deformities. Physiotherapists can be really helpful if there is anyone with specialist knowledge in your region. Ricky may also be interested in connecting with the Wellington Binder Exchange community on Facebook or the national free binder programme (https://bit.ly/33117Y8).
Sexual health and fertility
Discuss with Ricky any other immediate concerns, particularly around contraception and sexual health, and manage as appropriate. Ensure Ricky knows that, even if he is amenorrhoeic on testosterone, he is still potentially fertile and will require additional contraceptive when appropriate. Testosterone is contraindicated in pregnancy.
Though the long-term effects of GAHT are not yet clear, fertility may be affected. In Aotearoa, there is provision for funded sperm storage via local fertility services for those wanting to start feminising hormone therapy.
For Ricky, funded egg storage is not an option unless he were considering oophorectomy, but some places do offer a free fertility consultation to talk through private options, which he may want to take up. Inform him that while fertility is never guaranteed for anyone, many transmen have successfully stopped GAHT for the purposes of planned conception.
Voice changes
Funded vocal therapy may be an option in your region; if not, discuss accessing private speech language therapy as an alternative. However, for people starting masculinising hormones, the advice is to wait until they have been on GAHT for at least a year, during which time, their voice is likely to alter.
This is not the case for those starting feminising hormones, who can start vocal therapy at any stage of their transition.
Referral
After discussion with Ricky, he asks to be referred to your local GAHT provider.
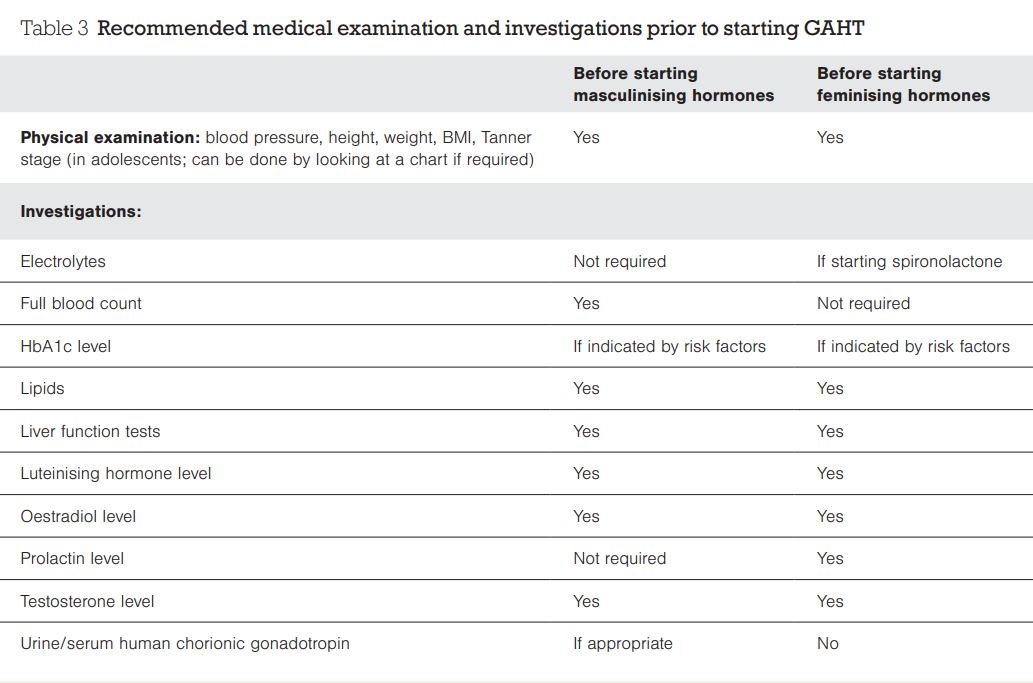
Before referring Ricky, ensure you have done everything on your referral “checklist”:
- blood tests and basic measurements, such as blood pressure, height and weight
- fertility discussions
- assess and support any mental health requirements/needs
- assess and manage any physical health issues
- assess ability to give informed consent (note that in some places, there may still be a requirement for a mental health provider to be involved in this part of the process).
Talk to Ricky about what he can expect from GAHT – we recommend using the consent forms for hormones as a discussion guide as they provide useful overviews of the treatment options, risks and side effects (download from https://bit.ly/2Ezxyn2).
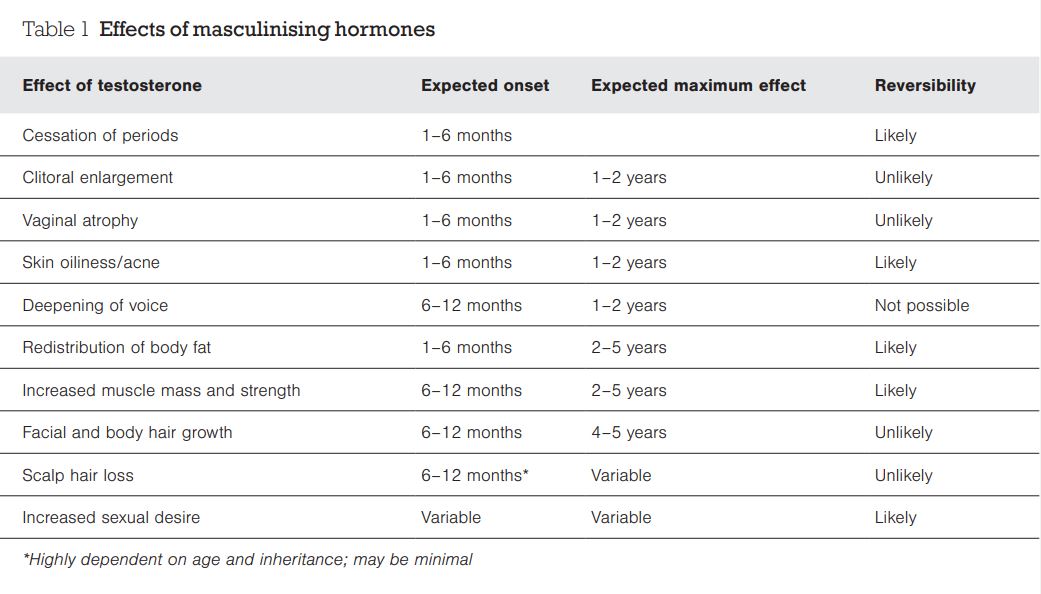
Ricky will be prescribed testosterone, usually via injections, with upwards titration of dose depending on physical changes and side effects.
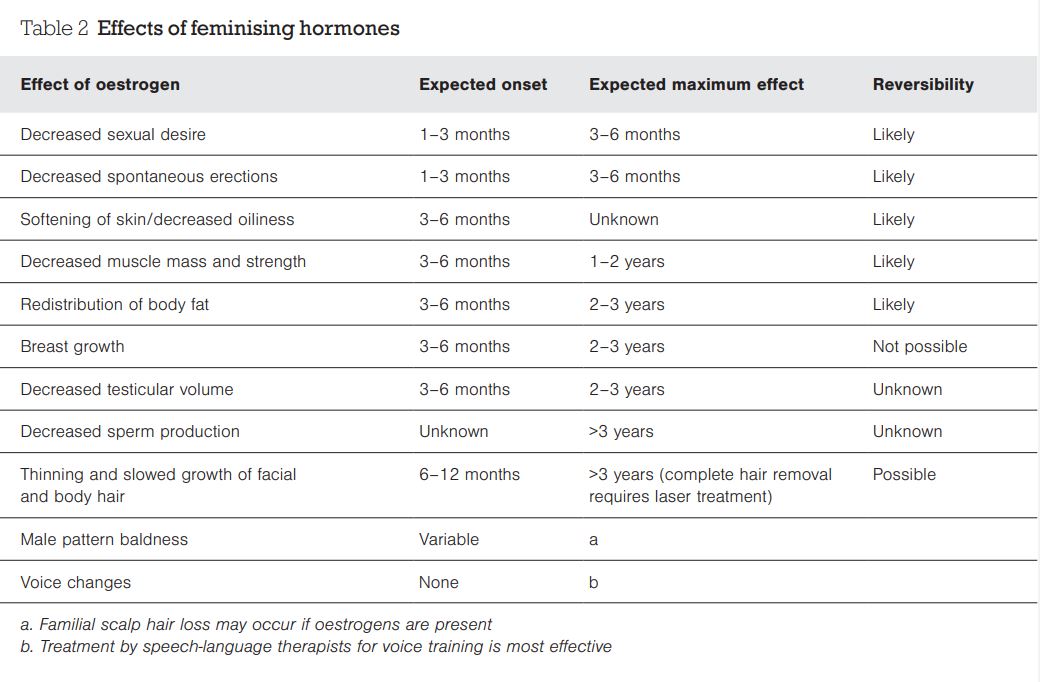
A patient wanting feminising hormones will be started on oestrogen – usually patches or tablets – but will also need an anti-androgen (eg, spironolactone, cyproterone or a gonadotropin-releasing hormone agonist) to counter the effects of their natural testosterone.
Note that transdermal oestrogen (patch) has a reduced risk of thromboembolic events and should be offered to everyone, but it is particularly indicated in the presence of increased thromboembolic risk, such as with increasing age, smoking, etc.
Offer Ricky support while he is waiting to be seen – in some areas, there may be a delay of several months or even more, which can be very difficult for patients with significant dysphoria or distress.











![Barbara Fountain, editor of New Zealand Doctor Rata Aotearoa, and Paul Hutchison, GP and senior medical clinician at Tāmaki Health [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/Barbara%20Fountain%2C%20editor%20of%20New%20Zealand%20Doctor%20Rata%20Aotearoa%2C%20and%20Paul%20Hutchison%2C%20GP%20and%20senior%20medical%20clinician%20at%20T%C4%81maki%20Health%20CR%20Simon%20Maude.jpg?itok=-HbQ1EYA)
![Lori Peters, NP and advanced health improvement practitioner at Mahitahi Hauora, and Jasper Nacilla, NP at The Terrace Medical Centre in Wellington [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/2.%20Lori%20Peters%2C%20NP%20and%20advanced%20HIP%20at%20Mahitahi%20Hauora%2C%20and%20Jasper%20Nacilla%2C%20NP%20at%20The%20Terrace%20Medical%20Centre%20in%20Wellington%20CR%20Simon%20Maude.jpg?itok=sUfbsSF1)
![Ministry of Social Development health and disability coordinator Liz Williams, regional health advisors Mary Mojel and Larah Takarangi, and health and disability coordinators Rebecca Staunton and Myint Than Htut [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/3.%20Ministry%20of%20Social%20Development%27s%20Liz%20Williams%2C%20Mary%20Mojel%2C%20Larah%20Takarangi%2C%20Rebecca%20Staunton%20and%20Myint%20Than%20Htut%20CR%20Simon%20Maude.jpg?itok=9ceOujzC)
![Locum GP Helen Fisher, with Te Kuiti Medical Centre NP Bridget Woodney [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/4.%20Locum%20GP%20Helen%20Fisher%2C%20with%20Te%20Kuiti%20Medical%20Centre%20NP%20Bridget%20Woodney%20CR%20Simon%20Maude.jpg?itok=TJeODetm)
![Ruby Faulkner, GPEP2, with David Small, GPEP3 from The Doctors Greenmeadows in Napier [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/5.%20Ruby%20Faulkner%2C%20GPEP2%2C%20with%20David%20Small%2C%20GPEP3%20from%20The%20Doctors%20Greenmeadows%20in%20Napier%20CR%20Simon%20Maude.jpg?itok=B0u4wsIs)
![Rochelle Langton and Libby Thomas, marketing advisors at the Medical Protection Society [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/6.%20Rochelle%20Langton%20and%20Libby%20Thomas%2C%20marketing%20advisors%20at%20the%20Medical%20Protection%20Society%20CR%20Simon%20Maude.jpg?itok=r52_Cf74)
![Specialist GP Lucy Gibberd, medical advisor at MPS, and Zara Bolam, urgent-care specialist at The Nest Health Centre in Inglewood [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/7.%20Specialist%20GP%20Lucy%20Gibberd%2C%20medical%20advisor%20at%20MPS%2C%20and%20Zara%20Bolam%2C%20urgent-care%20specialist%20at%20The%20Nest%20Health%20Centre%20in%20Inglewood%20CR%20Simon%20Maude.jpg?itok=z8eVoBU3)
![Olivia Blackmore and Trudee Sharp, NPs at Gore Health Centre, and Gaylene Hastie, NP at Queenstown Medical Centre [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/8.%20Olivia%20Blackmore%20and%20Trudee%20Sharp%2C%20NPs%20at%20Gore%20Health%20Centre%2C%20and%20Gaylene%20Hastie%2C%20NP%20at%20Queenstown%20Medical%20Centre%20CR%20Simon%20Maude.jpg?itok=Z6u9d0XH)
![Mary Toloa, specialist GP at Porirua and Union Community Health Service in Wellington, Mara Coler, clinical pharmacist at Tū Ora Compass Health, and Bhavna Mistry, specialist GP at Porirua and Union Community Health Service [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/9.%20Mary%20Toloa%2C%20Porirua%20and%20Union%20Community%20Health%20Service%20in%20Wellington%2C%20Mara%20Coler%2C%20T%C5%AB%20Ora%20Compass%20Health%2C%20and%20Bhavna%20Mistry%2C%20PUCHS%20CR%20Simon%20Maude.jpg?itok=kpChr0cc)