Life-limiting conditions can confront people with many challenges, up to and including death and dying. Dying affects all people, no matter who they are and what background they are from. Fair and universal access to humane and dignified support and services needs to be available. Enabling a way to provide timely access to medications for patients with distressing symptoms, where and when they need them, is a part of humane and dignified support and underpins the purpose of this proposed guideline.
Mortality and morbidity outcomes
Defining effectiveness in the context of a palliative and end-of-life-care guideline differs from a guideline with a curative model. Rather than reducing mortality, this guideline has a focus on improving the quality of life until death, and the quality of dying and death.
Reducing morbidity is as important in the palliative context as in any guideline. Interventions in a palliative care context need to reflect the desired outcomes of the individual and can include choices around antibiotics, transport to hospital and goals of care. More broadly, morbidity can include any health outcome that people experience and care about – physically or mentally.
This guideline promotes practices that support what individuals care about and are in their best interests. These can vary between patients because the guideline is patientfocused, but it is most effective when needs are identified and discussed early to enable informed choice.
Other outcome measures
Most clinical guidelines focus on the management of a single condition. The main weakness of this is the failure to address the impact of comorbid conditions, which are increasingly prevalent. The criteria for applying the anticipatory prescribing guideline are not condition specific, but rather, based on prognosis. It is applicable to a wide range of life-limiting conditions.
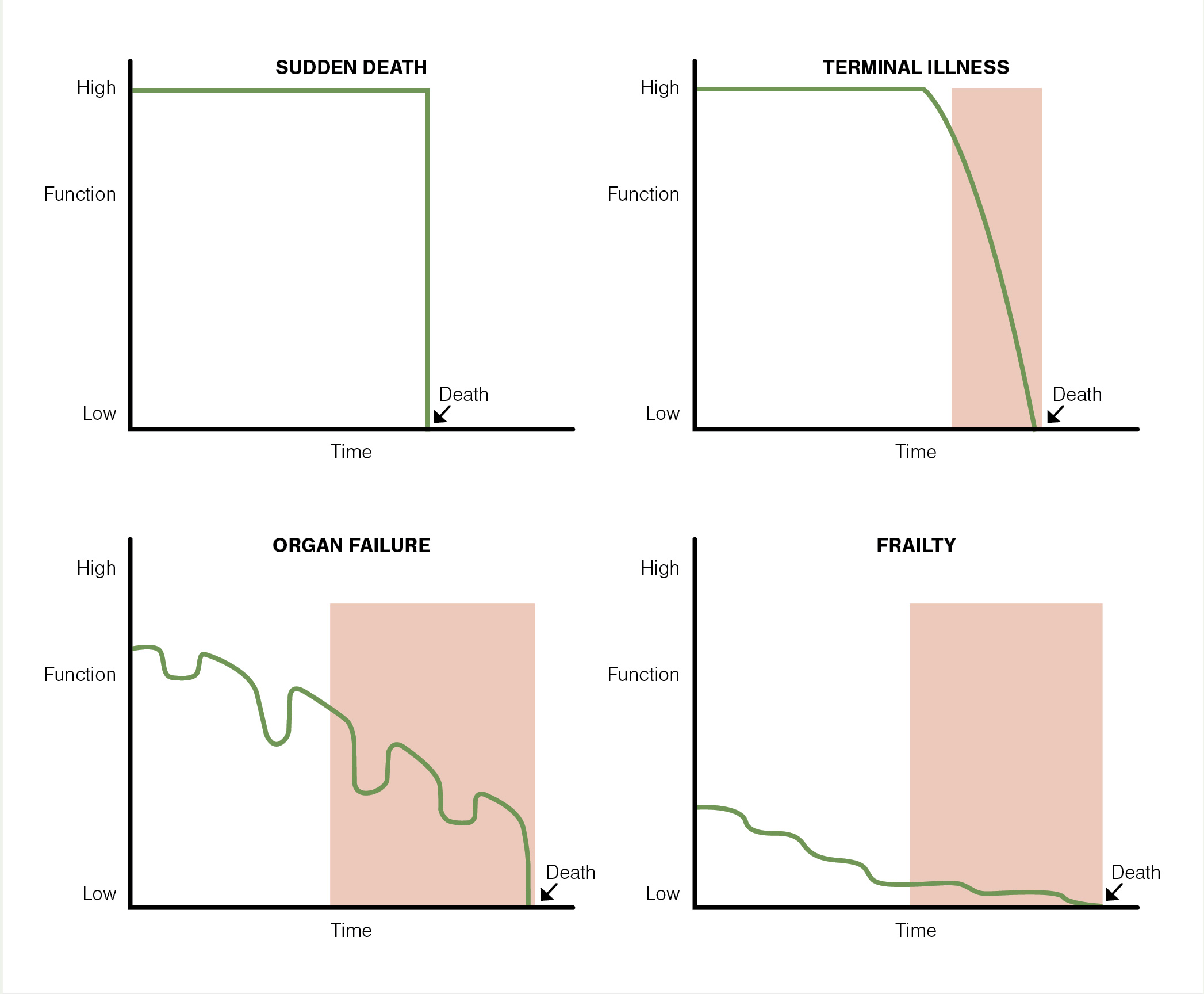
Since accurately predicting a time frame until death can be incredibly challenging, the guideline promotes the use of verified tools such as the Supportive and Palliative Care Indicators Tool (SPICT; spict.org.uk) or The Gold Standards Framework Proactive Identification Guidance (GSF PIG; tinyurl.com/GSF-PIG). The “When to initiate prescribing” figure (see above) may also be helpful. These tools can be used in conjunction with the “surprise question” approach – that is, would you be surprised if the patient were to die in the next year (or the next few months, weeks, days)?
Introducing the guideline
The draft guideline for “Anticipatory prescribing in community palliative and end-of-life care” is presented in the grey panel below. It presents a purpose, a criteria framework, a model of care, appropriate patient cohorts to consider, health professionals who can be involved, prescribing and dispensing considerations, and the sharing and management of information and care. Additionally, two patient scenarios are provided for context.
Resources that support the guideline
The guideline aims to facilitate prompt access to medications for patients experiencing distressing symptoms when and where they require them the most. This statement of purpose implies the when, what, why, where and how of the anticipatory prescribing intervention (Table 1).
With respect to the timing (when), medications must be prescribed in advance of the immediate need so they can be available in a timely way. To define what the purpose is, it is to provide medications to manage distressing symptoms. Relieving this distress, especially where harm can be predicted, represents the why. Where the patient is, generally being their usual place of residence, and in line with their wishes, demonstrates responsive patient-focused care. This is enabled (how) through an interdisciplinary team who are available to respond at any time and who can involve whānau/family in the process.
The elements outlined in the guideline are closely linked with the themes of key New Zealand documents and other clinical tools, and consistent with the strategic aims of the New Zealand Health Strategy, The New Zealand Palliative Care Strategy and several more (Table 1). The current healthcare reforms have the potential to further influence and shape these connections.
Developing high-quality, high-value, sustainable, equitable and patient-focused care are common aims of the strategies reflected in the practice guideline. Growing bodies of evidence contribute to clinical tools being developed, such as the SPICT and GSF PIG. These tools support early identification of palliative needs, which is linked with high-quality palliative care and improved patient experience. Identifying palliative needs early is a premise for prescribing anticipatory medications.
To ensure patients and whānau/family are represented in the process of when to prescribe, conversations around shared care approaches should be taking place, such as those in the Serious Illness Conversation Guide. This communication tool serves as a guide in the process of exploring a patient’s understanding of their illness, identifying their priorities and addressing concerns about future deteriorations in their health. It facilitates a thoughtful exploration before clinicians make recommendations, taking into account the patient’s values and the available interventions. Anticipatory prescribing may be discussed as a recommendation, and more than once if it is introduced early in the patient’s journey.
This communication approach is likely to alleviate some of the reported confusion among patients regarding the purpose of anticipatory medications.2









![Barbara Fountain, editor of New Zealand Doctor Rata Aotearoa, and Paul Hutchison, GP and senior medical clinician at Tāmaki Health [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/Barbara%20Fountain%2C%20editor%20of%20New%20Zealand%20Doctor%20Rata%20Aotearoa%2C%20and%20Paul%20Hutchison%2C%20GP%20and%20senior%20medical%20clinician%20at%20T%C4%81maki%20Health%20CR%20Simon%20Maude.jpg?itok=-HbQ1EYA)
![Lori Peters, NP and advanced health improvement practitioner at Mahitahi Hauora, and Jasper Nacilla, NP at The Terrace Medical Centre in Wellington [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/2.%20Lori%20Peters%2C%20NP%20and%20advanced%20HIP%20at%20Mahitahi%20Hauora%2C%20and%20Jasper%20Nacilla%2C%20NP%20at%20The%20Terrace%20Medical%20Centre%20in%20Wellington%20CR%20Simon%20Maude.jpg?itok=sUfbsSF1)
![Ministry of Social Development health and disability coordinator Liz Williams, regional health advisors Mary Mojel and Larah Takarangi, and health and disability coordinators Rebecca Staunton and Myint Than Htut [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/3.%20Ministry%20of%20Social%20Development%27s%20Liz%20Williams%2C%20Mary%20Mojel%2C%20Larah%20Takarangi%2C%20Rebecca%20Staunton%20and%20Myint%20Than%20Htut%20CR%20Simon%20Maude.jpg?itok=9ceOujzC)
![Locum GP Helen Fisher, with Te Kuiti Medical Centre NP Bridget Woodney [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/4.%20Locum%20GP%20Helen%20Fisher%2C%20with%20Te%20Kuiti%20Medical%20Centre%20NP%20Bridget%20Woodney%20CR%20Simon%20Maude.jpg?itok=TJeODetm)
![Ruby Faulkner, GPEP2, with David Small, GPEP3 from The Doctors Greenmeadows in Napier [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/5.%20Ruby%20Faulkner%2C%20GPEP2%2C%20with%20David%20Small%2C%20GPEP3%20from%20The%20Doctors%20Greenmeadows%20in%20Napier%20CR%20Simon%20Maude.jpg?itok=B0u4wsIs)
![Rochelle Langton and Libby Thomas, marketing advisors at the Medical Protection Society [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/6.%20Rochelle%20Langton%20and%20Libby%20Thomas%2C%20marketing%20advisors%20at%20the%20Medical%20Protection%20Society%20CR%20Simon%20Maude.jpg?itok=r52_Cf74)
![Specialist GP Lucy Gibberd, medical advisor at MPS, and Zara Bolam, urgent-care specialist at The Nest Health Centre in Inglewood [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/7.%20Specialist%20GP%20Lucy%20Gibberd%2C%20medical%20advisor%20at%20MPS%2C%20and%20Zara%20Bolam%2C%20urgent-care%20specialist%20at%20The%20Nest%20Health%20Centre%20in%20Inglewood%20CR%20Simon%20Maude.jpg?itok=z8eVoBU3)
![Olivia Blackmore and Trudee Sharp, NPs at Gore Health Centre, and Gaylene Hastie, NP at Queenstown Medical Centre [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/8.%20Olivia%20Blackmore%20and%20Trudee%20Sharp%2C%20NPs%20at%20Gore%20Health%20Centre%2C%20and%20Gaylene%20Hastie%2C%20NP%20at%20Queenstown%20Medical%20Centre%20CR%20Simon%20Maude.jpg?itok=Z6u9d0XH)
![Mary Toloa, specialist GP at Porirua and Union Community Health Service in Wellington, Mara Coler, clinical pharmacist at Tū Ora Compass Health, and Bhavna Mistry, specialist GP at Porirua and Union Community Health Service [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/9.%20Mary%20Toloa%2C%20Porirua%20and%20Union%20Community%20Health%20Service%20in%20Wellington%2C%20Mara%20Coler%2C%20T%C5%AB%20Ora%20Compass%20Health%2C%20and%20Bhavna%20Mistry%2C%20PUCHS%20CR%20Simon%20Maude.jpg?itok=kpChr0cc)