Some patients find the procedure more comfortable due to the curved compression plate and slightly reduced compression
Digital breast tomosynthesis (DBT or, as some know it, 3D mammography) is the latest digital breast imaging technology.
It uses a high-resolution mammogram technique where images of 1mm slices are acquired as the x-ray tube moves through an arc over the compressed breast. DBT was designed to overcome the limitations of full-field digital mammography (FFDM or 2D mammography).
DBT allows us to obtain multiple (the number of images depends on the breast size) high-resolution images of the breast, instead of the usual four images of FFDM (craniocaudal and mediolateral oblique views of each breast). It’s like having a mini-CT scan of the breast, but with much less radiation and better breast imaging resolution.
The biggest benefit of DBT over FFDM is that it prevents overlap of normal fibroglandular breast tissue. This is important as it prevents normal breast tissue from obscuring a breast cancer.
With FFDM, a breast cancer will appear as an irregular white mass against the normal fibroglandular tissue, which also appears white. Due to this lack of contrast, especially with denser breasts, the “white” fibroglandular tissue can overlap and obscure the “white” cancer, reducing breast cancer detection.
DBT is also important in reducing the number of pseudolesions (false positives) created by overlapping of normal fibroglandular tissue, which can make an area on the 2D mammogram look like there is a cancer when there is none, and will usually need further imaging to confirm normal appearances.
This creates anxiety and involves further exposure to radiation due to the need for extra views. By using DBT, extra views are not needed, which not only reduces the overall radiation dose but also improves patient psychology relating to their screening experience.
Another benefit of DBT is the ability to assess margins of lesions. DBT has been found to increase detection of invasive cancer (as many as 34–40 per cent more cancers detected than traditional mammography1), which is usually seen on a mammogram as an irregular, spiculated mass with surrounding architectural distortion. Due to the reduced overlap of normal breast tissue, these margins are more clearly seen.
DBT also allows us to assess benign masses, which look like a regular mass with smooth margins. Sometimes, we can also see fatty content in masses that are intramammary lymph nodes or breast hamartomas.
The procedure of obtaining a DBT is very similar to a 2D mammogram – the breast will be compressed in a similar manner. However, some patients find the procedure more comfortable due to the curved compression plate and slightly reduced compression compared with 2D mammography.
Because DBT has mainly a continuous arc movement over the breast, it can take a few seconds longer than a 2D mammogram, depending on the size of the breast (usually 30 to 40 seconds).
If performed as a stand-alone examination, the radiation dose of DBT is similar to 2D mammography.
The radiation dose of a mammogram is so small that the benefits of the examination outweigh the radiation risk. Therefore, DBT is considered an appropriate screening and diagnostic tool for detecting breast cancer.
One of the disadvantages of using DBT for screening is cost, which is greater than for 2D mammography due to costs of the equipment, digital storage of multiple images, and increased reading times for radiologists because of the multiple images. Since these extra costs are not completely covered by certain health insurers, patients are often asked to pay a supplementary fee (approximately $100).
Some studies have found DBT does not increase detection of ductal carcinoma in situ (DCIS) as the calcifications are better characterised on 2D imaging. Many vendors have improved the synthesised 2D images that are obtained from the 3D stack, without extra radiation, to allow better assessment for calcifications and DCIS.
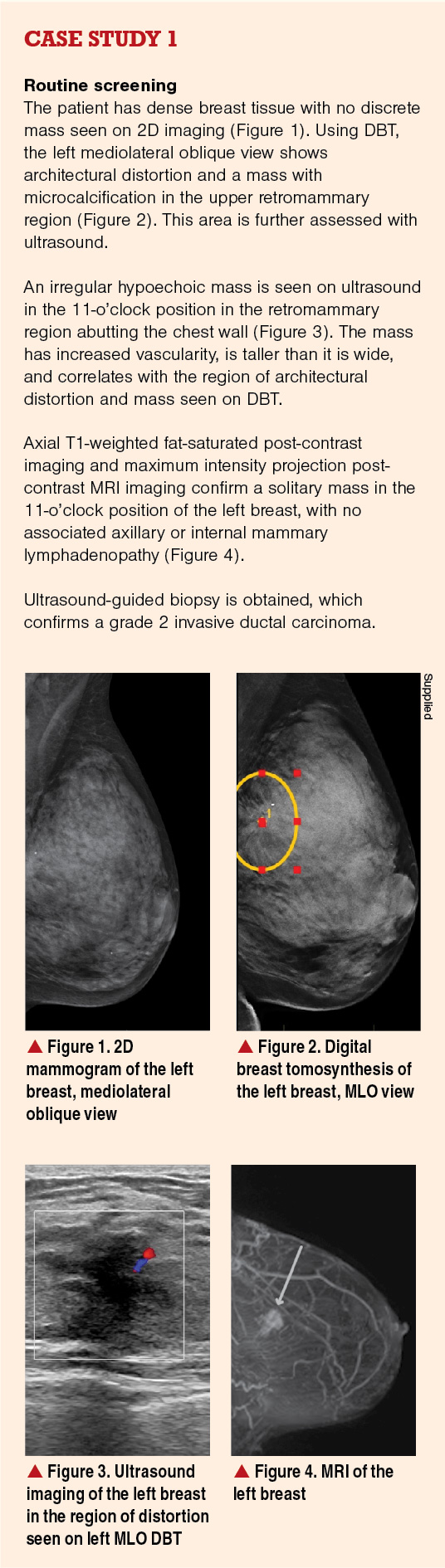
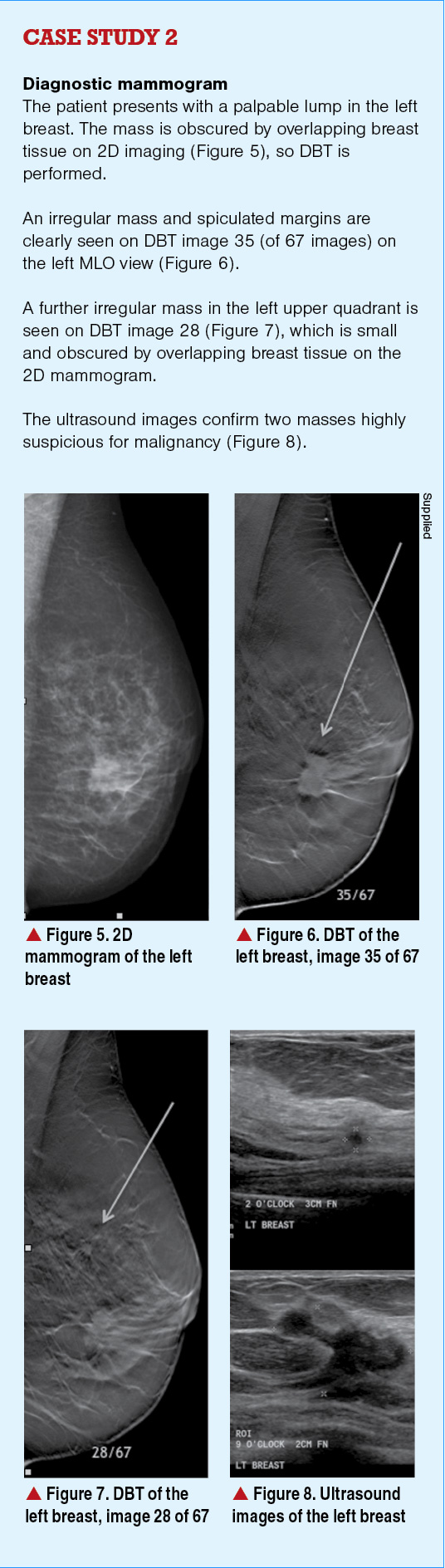
DBT is fast becoming the standard of mammography, being effective in both screening (asymptomatic women; see case study 1) and diagnostic (symptomatic women; see case study 2) settings, with the potential to replace standard 2D mammography in the future.






![Barbara Fountain, editor of New Zealand Doctor Rata Aotearoa, and Paul Hutchison, GP and senior medical clinician at Tāmaki Health [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/Barbara%20Fountain%2C%20editor%20of%20New%20Zealand%20Doctor%20Rata%20Aotearoa%2C%20and%20Paul%20Hutchison%2C%20GP%20and%20senior%20medical%20clinician%20at%20T%C4%81maki%20Health%20CR%20Simon%20Maude.jpg?itok=-HbQ1EYA)
![Lori Peters, NP and advanced health improvement practitioner at Mahitahi Hauora, and Jasper Nacilla, NP at The Terrace Medical Centre in Wellington [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/2.%20Lori%20Peters%2C%20NP%20and%20advanced%20HIP%20at%20Mahitahi%20Hauora%2C%20and%20Jasper%20Nacilla%2C%20NP%20at%20The%20Terrace%20Medical%20Centre%20in%20Wellington%20CR%20Simon%20Maude.jpg?itok=sUfbsSF1)
![Ministry of Social Development health and disability coordinator Liz Williams, regional health advisors Mary Mojel and Larah Takarangi, and health and disability coordinators Rebecca Staunton and Myint Than Htut [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/3.%20Ministry%20of%20Social%20Development%27s%20Liz%20Williams%2C%20Mary%20Mojel%2C%20Larah%20Takarangi%2C%20Rebecca%20Staunton%20and%20Myint%20Than%20Htut%20CR%20Simon%20Maude.jpg?itok=9ceOujzC)
![Locum GP Helen Fisher, with Te Kuiti Medical Centre NP Bridget Woodney [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/4.%20Locum%20GP%20Helen%20Fisher%2C%20with%20Te%20Kuiti%20Medical%20Centre%20NP%20Bridget%20Woodney%20CR%20Simon%20Maude.jpg?itok=TJeODetm)
![Ruby Faulkner, GPEP2, with David Small, GPEP3 from The Doctors Greenmeadows in Napier [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/5.%20Ruby%20Faulkner%2C%20GPEP2%2C%20with%20David%20Small%2C%20GPEP3%20from%20The%20Doctors%20Greenmeadows%20in%20Napier%20CR%20Simon%20Maude.jpg?itok=B0u4wsIs)
![Rochelle Langton and Libby Thomas, marketing advisors at the Medical Protection Society [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/6.%20Rochelle%20Langton%20and%20Libby%20Thomas%2C%20marketing%20advisors%20at%20the%20Medical%20Protection%20Society%20CR%20Simon%20Maude.jpg?itok=r52_Cf74)
![Specialist GP Lucy Gibberd, medical advisor at MPS, and Zara Bolam, urgent-care specialist at The Nest Health Centre in Inglewood [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/7.%20Specialist%20GP%20Lucy%20Gibberd%2C%20medical%20advisor%20at%20MPS%2C%20and%20Zara%20Bolam%2C%20urgent-care%20specialist%20at%20The%20Nest%20Health%20Centre%20in%20Inglewood%20CR%20Simon%20Maude.jpg?itok=z8eVoBU3)
![Olivia Blackmore and Trudee Sharp, NPs at Gore Health Centre, and Gaylene Hastie, NP at Queenstown Medical Centre [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/8.%20Olivia%20Blackmore%20and%20Trudee%20Sharp%2C%20NPs%20at%20Gore%20Health%20Centre%2C%20and%20Gaylene%20Hastie%2C%20NP%20at%20Queenstown%20Medical%20Centre%20CR%20Simon%20Maude.jpg?itok=Z6u9d0XH)
![Mary Toloa, specialist GP at Porirua and Union Community Health Service in Wellington, Mara Coler, clinical pharmacist at Tū Ora Compass Health, and Bhavna Mistry, specialist GP at Porirua and Union Community Health Service [Image: Simon Maude]](/sites/default/files/styles/thumbnail_cropped_100/public/2025-03/9.%20Mary%20Toloa%2C%20Porirua%20and%20Union%20Community%20Health%20Service%20in%20Wellington%2C%20Mara%20Coler%2C%20T%C5%AB%20Ora%20Compass%20Health%2C%20and%20Bhavna%20Mistry%2C%20PUCHS%20CR%20Simon%20Maude.jpg?itok=kpChr0cc)